1. Trauma: ie, trauma, chronic contact lens use, chronic rubbing of the eye, etc.
2. Sun exposure: excessive sun exposure without eye protection can lead to pingueculas or pterygia which I have now seen begin to destroy meibomian glands. I recommend removal of these growths asap so they do not lead to chronic dry eye in the future.
3. Inflammation: ie, from rosacea, from chronic allergies, from a bad diet (this last one is my theory only & has not been proven yet directly to be associated with MGD but I hypothesize it is)
4. Mutation: ie cancer, radiation, chemo
5. Genetics:
—>LEADS to more inflammation which leads to more meibomian gland inflammation which leads to loss of glands which can lead to dry eye symptoms and even corneal scar tissue…which can even lead to a loss of vision requiring a corneal transplant: a full corneal transplant (not just DMEK or DSEK or DSAEK)[** definitions are below]
It becomes a vicious cycle.
Here is a 16 year old patient who had a large papilloma on her right eye caruncle: photo coming soon.
We excised it as it was large, but it looks like the growth destroyed all the upper eyelid’s meibomian glands. Or an alternative hypothesis: the loss of all the Right Upper Lid meibomian glands led to the growth of the large papilloma. Which came first? Not sure, but I am pretty sure the growth made the glands worse also.
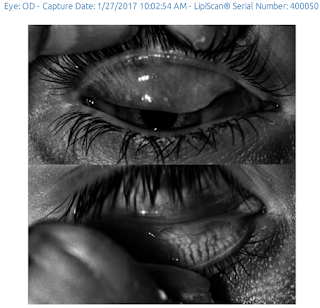
Here is the Right Upper Lid: there are almost no meibomian glands left; Her lower lid is shown below as a finger was in the way of #1:
1.


Above is left upper and lower lid: not terribly abnormal.
Below is pathology report: final diagnosis Squamos Papilloma.

[** definitions are below]

If the stroma or anterior cornea is scarred, a full PK will be needed which is what I am seeing in kids with severe corneal scar tissue and severe meibomian gland atrophy.
With Fuchs’ endothelial dystrophy or when there is swelling of the cornea after cataract surgery, it is the endothelium which is compromised: some of these patients need a DMEK or DSEK.