My father-in-law, from the Netherlands, had debilitating sensations of imbalance and vertigo a few years ago when I was teaching at Harvard Medical School. We found a wonderful therapist who really saved him. Her name is Janet Callahan and she is at MGH in Boston. Since then, my father, a cardiothoracic surgeon, swears by the following short cut to get rid of vertigo. It may not help everyone but it should not make you worse: at least he says no one has been made worse by this and it helps: this has not been published so be careful not to fall out of your chair when doing this.Quick Treatment for Vertigo: Dr. Fernando Lora’s The Lora Maneuver1. Drink plenty of water: more than 64oz of water a day. Do not drink soda, caffeine, or anything else that will dehydrate you or increase your inflammation. Do this daily.2. Be sure you are seated in a safe location when you do the following. When you feel dizzy: take a little breath, use each hand to close your ear and nostril at the same time (thus both ears and both nostrils are closed with your hands: just open your hand wide, put your thumbs to close your ears and your pinkie or 4th fingers to close your nostrils) & then before you need to take another breath move your whole head (just your head) in big circles 10 times to the right and then 10 times to the left. Keep doing this until dizziness goes away. At first try a couple of times.3. You may feel more dizzy when you do this so do not fall out of your chair. Doing this a few times will help re-establish and reposition your semicircular canal canaliths which can get stuck and cause vertigo. This is a form of Canalith repositioning which is easy to do. The Epley Maneuver can also help, but the above Lora Maneuver is safer in my opinion and can be done without the help of any body. Epley Maneuver
Below is a great review from Up To Date:INTRODUCTION
Dizziness is a feeling that may be hard to describe, but often includes a feeling that you are spinning or tilting, or that you are about to fall or pass out. Dizziness can also cause you to feel lightheaded or giddy, or have difficulty walking straight.
Many people who feel dizzy have vertigo, a specific type of dizziness. Vertigo causes a sense of spinning dizziness, swaying, or tilting. You may feel that you are moving or that the room is moving around you. Vertigo can be caused by a number of different problems involving the inner ear or brain. Some of these problems are not serious while others can be life threatening.
The most common symptoms of vertigo include a feeling of:
Spinning (you or the room around you)
Tilting or swaying
Feeling off balance
These feelings come and go, and may last seconds, hours, or days. You may feel worse when you move your head, change positions (stand up, roll over), cough, or sneeze. Along with vertigo, you may:
Vomit or feel nauseous
Have a headache or be sensitive to light and noise
See double, have trouble speaking or swallowing, or feel weak
Feel short of breath or sweaty, have a racing heart beat
If you seek treatment for vertigo, you should mention how long these symptoms last, what triggers the symptoms, and any other associated problems. These clues can help point to the cause of vertigo.
COMMON CAUSES OF VERTIGO
The most common causes of vertigo include:
Inner ear problems — Collections of calcium, inflammation, and certain infections can cause problems in the vestibular system. The vestibular system includes parts of the inner ear and nervous system, which controls balance (figure 1). Benign paroxysmal positional vertigo, Meniere disease, and vestibular neuritis are three of the most common types of vertigo caused by inner ear problems.
Benign paroxysmal positional vertigo (BPPV) — BPPV, sometimes called benign positional vertigo, positional vertigo, postural vertigo, or simply vertigo, is a type of vertigo that develops due to collections of calcium in the inner ear. These collections are called canaliths. Moving the canaliths (called canalith repositioning) is a common treatment for BPPV. Vertigo is typically brief in people with BPPV, lasting seconds to minutes. Vertigo can be triggered by moving the head in certain ways. (See “Benign paroxysmal positional vertigo”.)
Meniere disease — Meniere disease is condition that causes repeated spells of vertigo, hearing loss, and ringing in the ears. Spells can last several minutes or hours. It is probably caused by a buildup of fluid in the inner ear. (See “Meniere disease”.)
Vestibular neuritis — Vestibular neuritis, also known as labyrinthitis, is probably caused by a virus that causes swelling around the balance nerve. People with vestibular neuritis develop sudden, severe vertigo, nausea, vomiting, and difficulty walking or standing up; these problems can last several days. Some people also develop difficulty hearing in one ear. (See “Vestibular neuritis”.)
Medications — Rarely, medications can actually damage the inner ear. Other medications can affect the function of the inner ear or brain and lead to vertigo.
Migraines — In a condition called vestibular migraine or migrainous vertigo, vertigo can be caused by a migraine. This type of vertigo usually happens along with a headache, although sometimes there is no headache. (See “Vestibular migraine”.)
Brain problems, such as a stroke or TIA (transient ischemic attack), bleeding in the brain, or multiple sclerosis can also cause vertigo. There are usually other symptoms, besides vertigo, that happen with these brain problems. (See “Pathophysiology, etiology, and differential diagnosis of vertigo”.)
WHEN TO SEEK HELP
You should seek help immediately if you have dizziness or vertigo along with any of the following:
New or severe headache
Temperature greater than 100.4ºF (38ºC)
Seeing double or having trouble seeing clearly
Trouble speaking or hearing
Weakness in an arm or leg
An inability to walk without assistance
Passing out
Numbness or tingling
Chest pain
Vomiting that will not stop
In addition, you should seek help immediately if you have vertigo that lasts for several minutes or more if you:
Are an older adult
Have had a stroke in the past
Have risk factors for stroke (high blood pressure, diabetes, smoking)
If you have dizziness or vertigo that comes and goes but you do not have any of the above problems, make an appointment with your doctor or nurse. He or she will perform a physical exam, and may order further testing, depending on your exam and medical history.
VERTIGO TREATMENT
In most people, vertigo is bothersome but it is not caused by a serious problem. Treatment for vertigo aims to treat the underlying cause (if the cause is known), relieve the bothersome symptoms, and help with recovery. This section will discuss treatment for symptoms and treatments to help with recovery.
Treatment for symptoms — If you have spells of vertigo that are severe or last for hours or days, your doctor or nurse may recommend a medication to relieve severe vertigo symptoms, like vomiting. Treatment with medication is not usually recommended if your vertigo lasts only second or minutes.
Possible medication treatments include:
An antihistamine, such as the prescription medicine meclizine (Antivert®), or non-prescription medicines like dimenhydrinate (Dramamine®), or diphenhydramine (Benadryl®).
Prescription anti-nausea medicines, such as promethazine (Phenergan®), metoclopramide (Reglan®), or ondansetron (Zofran®).
Prescription sedative medicines, such as diazepam (Valium®), lorazepam (Ativan®), or clonazepam (Klonopin®)
Most of these medicines make you sleepy, and you should not take them before you work or drive. You should only take prescription medicines to treat severe vertigo symptoms, and you should stop the medicine when your symptoms improve.
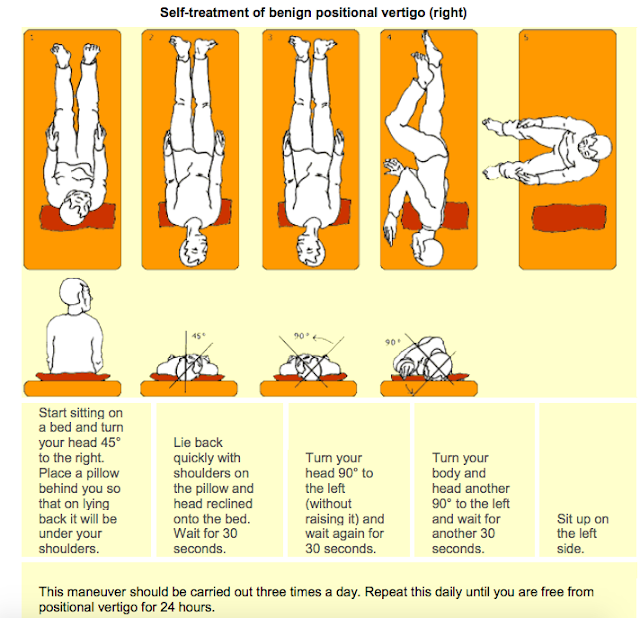
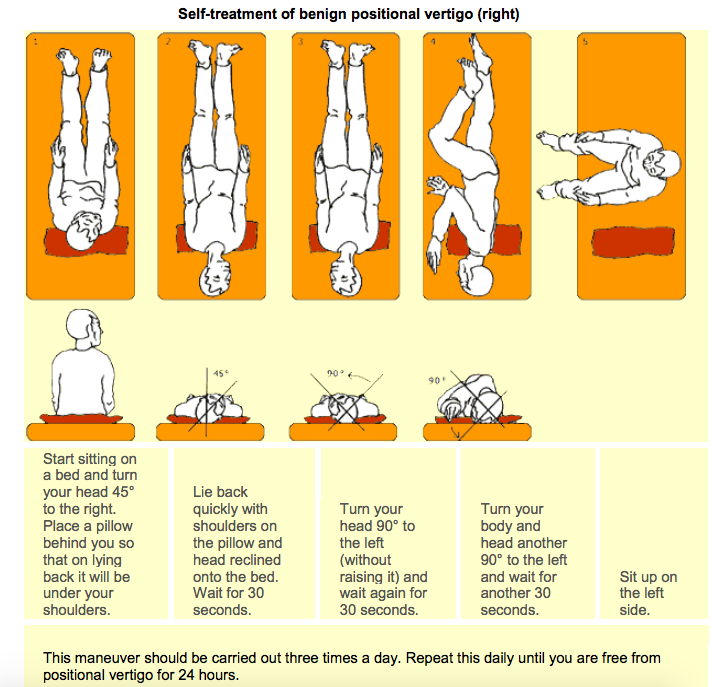
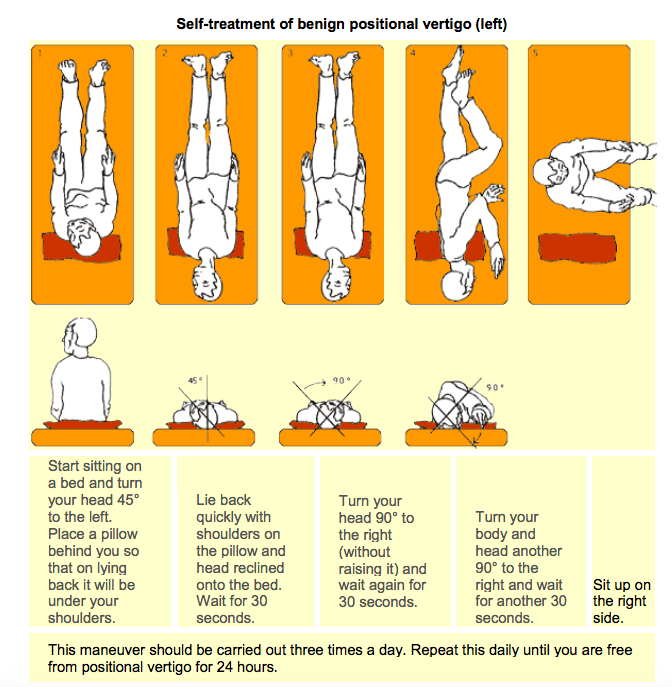
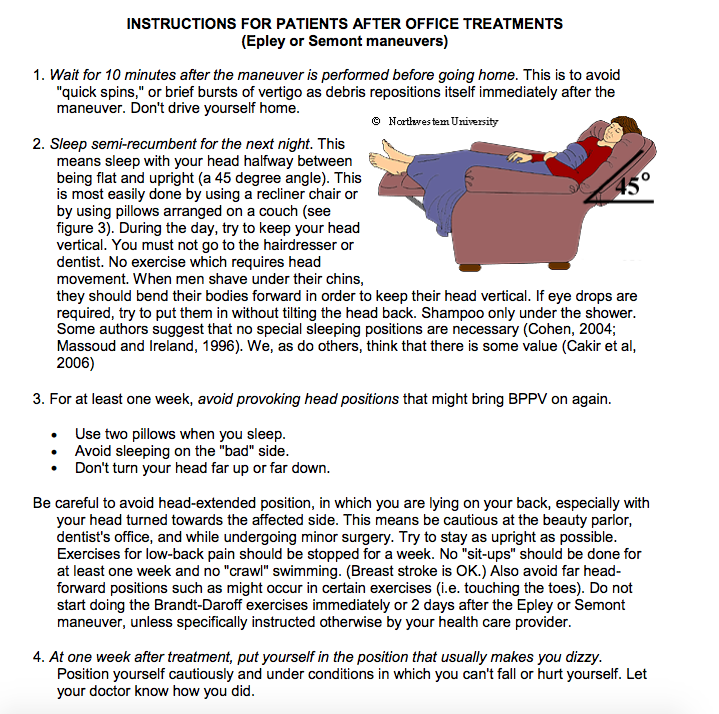
Canalith repositioning — Canalith repositioning is a treatment that may be recommended for people with benign paroxysmal positional vertigo (BPPV). The treatment will be done by a doctor, nurse, or therapist in the office by moving your head into certain positions, sometimes called the Epley maneuver. You may be given instructions on how to perform similar movements at home, if needed.
These movements encourage the calcium collection to move into a part of the ear where it will be reabsorbed. You may begin to feel better immediately after this treatment or within a day or two.
Balance rehabilitation — Most patients with vertigo prefer to keep their head still. However, staying still and not moving your head can make it harder to cope with vertigo. Rehabilitation can help people with vertigo that is caused by injury to the vestibular system. The vestibular system includes parts of the inner ear and nervous system, which controls balance.
The rehabilitation works by helping your brain adjust its response to changes in the vestibular system. The therapy can also help train your eyes and other senses to “learn” how to compensate. This therapy is most helpful when it is started as soon as possible after you develop vertigo.
During rehabilitation, you will work with a therapist who will teach to you perform exercises at home. For example, you might start by focusing on an object with a blank background and move your head slowly to the right and left and up and down. You would perform this exercise for several minutes two to three times per day.
If you have trouble standing or walking because of vertigo, you are at risk for falling. In older adults, falls can lead to serious complications, such as a broken hip. Talk to your doctor, nurse, or therapist about your concerns. To reduce the risk of falls, get rid of hazards in your home, such as loose electrical cords and slippery rugs, and avoid walking in unfamiliar areas that are not lighted.
WHERE TO GET MORE INFORMATION
Your healthcare provider is the best source of information for questions and concerns related to your medical problem.
This article will be updated as needed on our web site (www.uptodate.com/patients). Related topics for patients, as well as selected articles written for healthcare professionals, are also available. Some of the most relevant are listed below.
Patient level information — UpToDate offers two types of patient education materials.
The Basics — The Basics patient education pieces answer the four or five key questions a patient might have about a given condition. These articles are best for patients who want a general overview and who prefer short, easy-to-read materials.
Beyond the Basics — Beyond the Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are best for patients who want in-depth information and are comfortable with some medical jargon.
This topic currently has no corresponding Beyond the Basics content.
Professional level information — Professional level articles are designed to keep doctors and other health professionals up-to-date on the latest medical findings. These articles are thorough, long, and complex, and they contain multiple references to the research on which they are based. Professional level articles are best for people who are comfortable with a lot of medical terminology and who want to read the same materials their doctors are reading.