Many people are working around the clock to find the best treatment option for COVID. I was speaking recently to a friend about how his shift starts at 4am for the for the COVID vaccine trials he is involved in.
Everyone needs to do some research to see what you are comfortable with trying or using if your MD recommends this.
If the goal is to save the most vulnerable of the population, then we have no choice but to encourage herd immunity until a safe, proven vaccine is available which could take many more months and even years. To achieve herd immunity, usually, 70% of the healthy population need to get the virus to develop antibodies in order to protect others.
Below are also the sheets discussed in this video.
Personally, I think Hydroxychloroquine works to treat COVID-19 and as a prophylaxis (to prevent or decrease COVID-19’s viral load). I would try personally, though, to prevent COVID with diluted-povidone-iodine or 70% alcohol gargles as mentioned in video below.
Here is a good website with all the possible treatment options for active COVID-19 infections.
https://covid-19tracker.milkeninstitute.org/#treatment_antibodies
Covid 19 treatment
THIS IS AN UNPREDICTABLE EVOLVING UNKNOWN VIRUS WHICH GIVES SURPRISES AND TREATMENT PROTOCOLS MAY NEED TO BE CHANGED.
FOR TREATMENT WITH DIAGNOSIS OF COVID-19
OPTION 1
-AZITHROMYCIN 250 MG (ANTIBIOTIC) 2 TABLETS ON DAY AND THEN 1 TABLET DAILY FOR 4 DAYS
-HYDROXYCHLOROQUINE 200 MG 2 TABLETS TWICE DAILY ON
DAY 1, THEN 1 TABLET 200 MG TWICE DAILY FOR 7 DAYS
–VITAMIN C 2000 mg. DAILY
-VITAMIN D3 5000units DAILY
-ZINC
OPTION 2
-AZITHROMYCIN 250 MG 2 TABLETS ON DAY 1 AND THEN
1 TABLET DAILY FOR 4 DAYS
-DEXAMETHASONE 6 MG DAILY FOR 7 DAYS
-PLUS ALL VITAMINS DISCUSSED EARLIER
OPTION 3
-AZITHROMYCIN 250 MG 2 TABLETS ON DAY 1 AND THEN
1 TABLET DAILY FOR 4 DAYDS
-BUDESONIDE BY NEBULIZER 0.5 MG/2CC BY AEROSOL TWICE
DAILY FOR 7 DAYS (SOMETIMES A BIT LONGER)
-PLUS ALL VITAMINS DISCUSED EARLIER
FOR PREVENTION OF COVID IF THE PERSON IS EXPOSED TO THE PUBLIC
HYDROXYCHLOROQUINE 200 MG DAILY
PLUS ALL VITAMINS DISCUSSED EARLIER.
Dr. Cremers recommends diluted 5% Povidone Iodine and/or 70% alcohol gargling (& swabbing of nose with diluted cuetipes in PI or 70% ETOH) 4x/day if no allergies to iodine at first feeling of getting sick (ie sore throat, fever, headache with tingling in throat) or if exposed to a COVID-19 patient.
Convalescent Plasma is also an exciting option in treating patients.
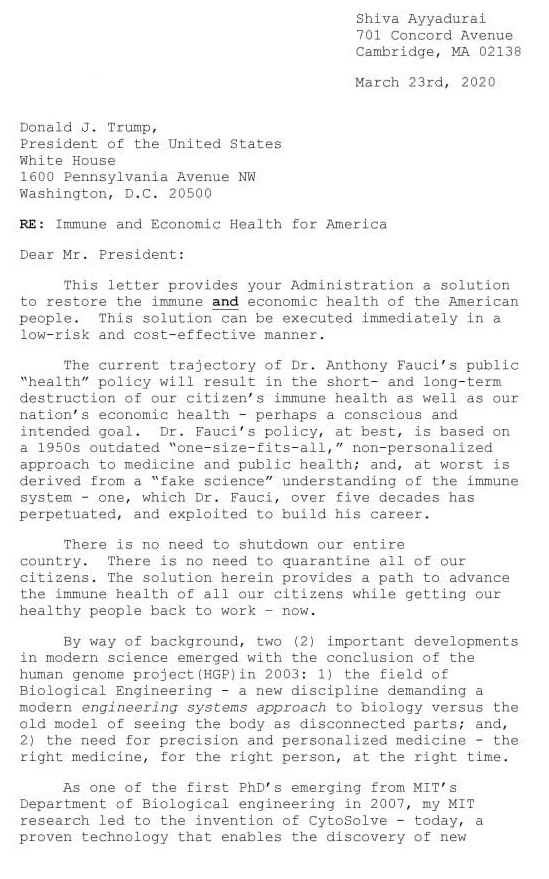
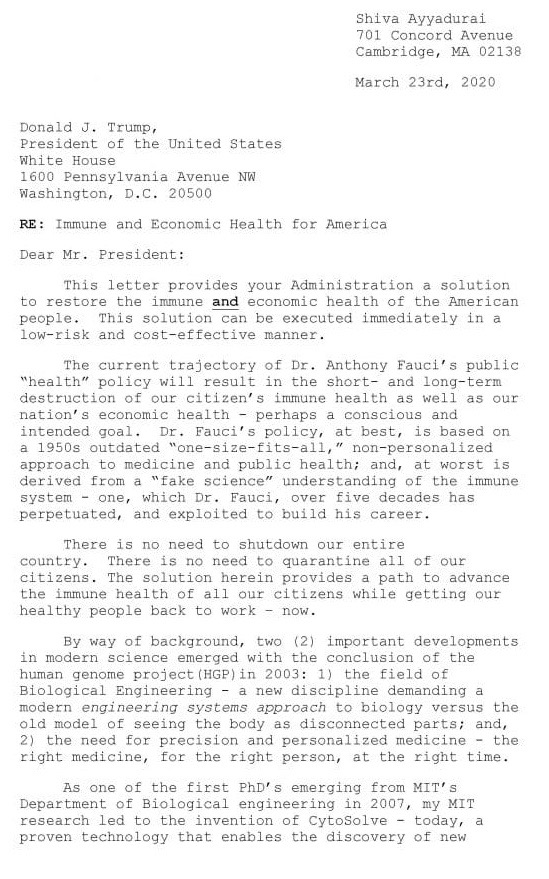
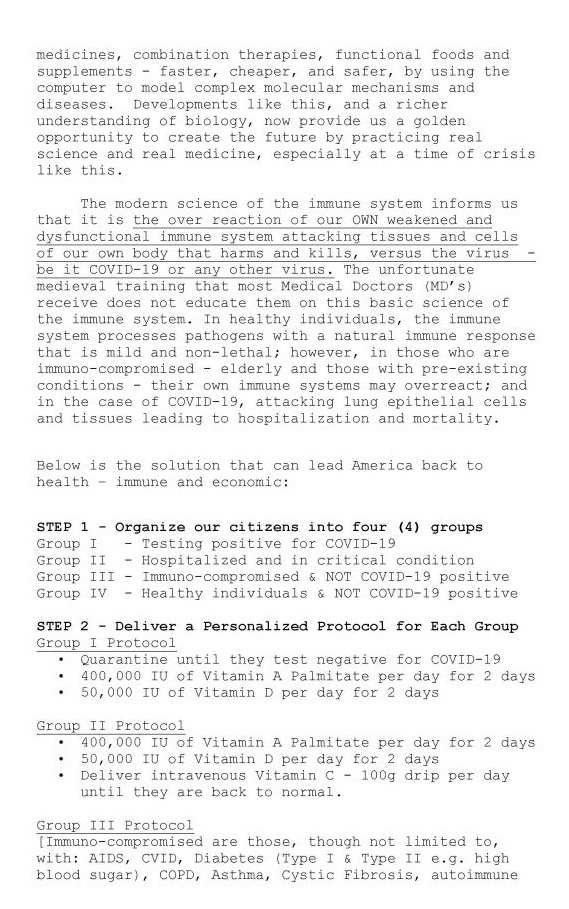
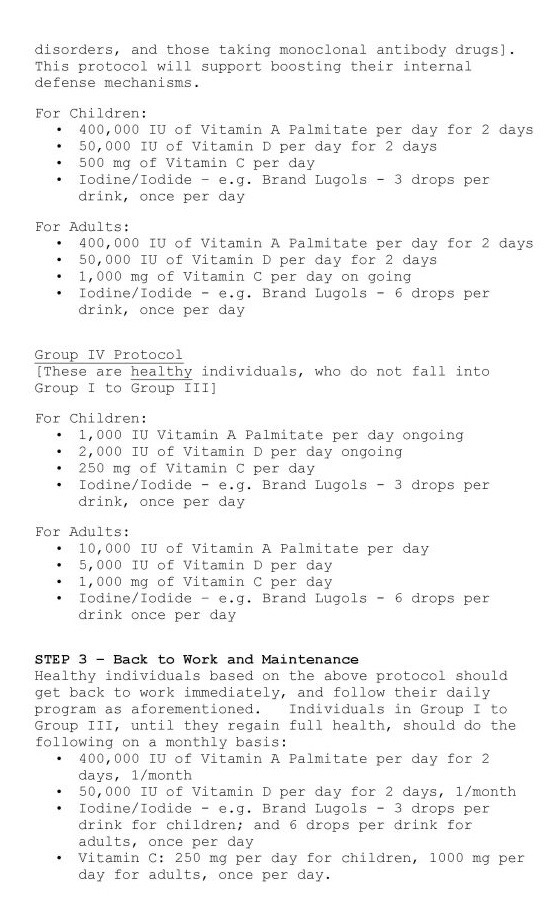
From: Dr. Shriva Ayyaduri
References:
Vitamin A, infection, and immune function
C B Stephensen. Annu Rev Nutr.2001.
infectious diseases can precipitate vitamin A deficiency by decreasing intake, decreasing absorption, and increasing excretion. Infectious diseases that induce the acute-phase response also impair the assessment of vitamin A status by transiently depressing serum retinol concentrations. Vitamin A deficiency impairs innate immunity by impeding normal regeneration of mucosal barriers damaged by infection, and by diminishing the function of neutrophils, macrophages, and natural killer cells. Vitamin A is also required for adaptive immunity and plays a role in the development of T both-helper (Th) cells and B-cells. In particular, vitamin A deficiency diminishes antibody-mediated responses directed by Th2 cells, although some aspects of Th1-mediated immunity are also diminished. These changes in mucosal epithelial regeneration and immune function presumably account for the increased mortality seen in vitamin A-deficient infants, young children, and pregnant women in many areas of the world today.
Major reduction of malaria morbidity with combined vitamin A and zinc supplementation in young children in Burkina Faso: a randomized double blind trial
Augustin N Zeba et al. Nutr J. 2008.
Background: Vitamin A and zinc are crucial for normal immune function, and may play a synergistic role for reducing the risk of infection including malaria caused by Plasmodium falciparum.
Methods: A randomized, double-blind, placebo-controlled trial of a single dose of 200 000 IU of vitamin A with daily zinc supplementation was done in children of Sourkoudougou village, Burkina Faso. Children aged from 6 to 72 months were randomized to receive a single dose of 200 000 IU of vitamin A plus 10 mg elemental zinc, six days a week (n = 74) or placebo (n = 74) for a period of six months. Cross-sectional surveys were conducted at the beginning and the end of the study, and children were evaluated daily for fever. Microscopic examination of blood smear was done in the case of fever (temperature > or =37.5 degrees C) for malaria parasite detection.
Results: At the end of the study we observed a significant decrease in the prevalence malaria in the supplemented group (34%) compared to the placebo group (3.5%) (p < 0.001). Malaria episodes were lower in the supplemented group (p = 0.029), with a 30.2% reduction of malaria cases (p = 0.025). Time to first malaria episode was longer in the supplemented group (p = 0.015). The supplemented group also had 22% fewer fever episodes than the placebo group (p = 0.030).
Conclusion: These results suggest that combined vitamin A plus zinc supplementation reduces the risk of fever and clinical malaria episodes among children, and thus may play a key role in malaria control strategies for children in Africa.
A randomized, controlled trial of vitamin A in children with severe measles
G D Hussey et al. N Engl J Med.1990.
As compared with the placebo group, the children who received vitamin A recovered more rapidly from pneumonia (mean, 6.3 vs. 12.4 days, respectively; P less than 0.001) and diarrhea (mean, 5.6 vs. 8.5 days; P less than 0.001), had less croup (13 vs. 27 cases; P = 0.03), and spent fewer days in the hospital (mean, 10.6 vs. 14.8 days; P = 0.01). Of the 12 children who died, 10 were among those given placebo (P = 0.05). For the group treated with vitamin A, the risk of death or a major complication during the hospital stay was half that of the control group (relative risk, 0.51; 95 percent confidence interval, 0.35 to 0.74).
Vitamin A as an immunomodulating agent
M M Rumore. Clin Pharm. 1993 Jul.
Measles may increase the body’s utilization of vitamin A, possibly because of the rapid destruction of epithelial surfaces. Vitamin A may boost immune responses in the elderly, persons with high exposure to ultraviolet light, patients who have undergone surgery, and persons with parasitic infection, but more studies are needed. The immune defect caused by vitamin A deficiency may be due to alterations in the glycoproteins of the lymphocyte membrane, an adverse effect on helper T-cell function, the effect on epithelial tissue, or some other mechanism. Vitamin A therapy is relatively safe, and its effectiveness in children with measles and possibly other groups appears to justify public health campaigns to eliminate vitamin A deficiency. Vitamin A apparently has important immunomodulating properties, notably in patients with measles.
Vitamin A as an anti-inflammatory agent
Ram Reifen. Proc Nutr Soc. 2002 Aug.
Supplementation with vitamin A has been found to be beneficial in a number of inflammatory conditions, including skin disorders such as acne vulgaris, broncho-pulmonary dysplasia and some forms of precancerous and cancer states. The present review suggests that vitamin A deficiency induces inflammation and aggravates existing inflammatory states. Supplementation with vitamin A in selected cases could ameliorate inflammation. The two main mechanisms which appear to be involved in the prevention of disease are the effects of vitamin A on the immune system and the effect on epithelial integrity.