MTHFR, short for Methylenetetrahydrofolate Reductase, is a very important enzyme in the body. This enzyme is necessary for Methylation to occur which is a metabolic process that switches genes on and off, repairs DNA and many other important things.
Methylation is also essential to convert both folate and folic acid – each a form of Vitamin B9 – into its active, usable form called 5-MTHF.
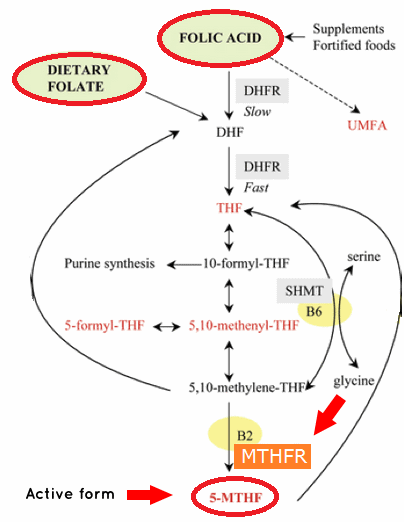
This is a diagram of how complex it is, but you only need to see the final step.
All the steps required to convert folate and folic acid into their active form, 5-MTHF
You can see that the final (bottom) step requires MTHFR in order to create the active form.
So without the enzyme activity of MTHFR, methylation of folate and folic acid cannot occur properly.
MTHFR gene
Put simply, the MTHFR gene triggers the production of MTHFR enzymes.
Think of the gene as the flower, the enzyme as the honey-bee, and active folic acid as honey.
How to Get Tested for a MTHFR Mutation?
Methylenetetrahydrofolate Reductase test has become popular due its potential to uncover some important health risk factors as well as explain some mysterious symptoms you may have been struggling with for years.
If you have any of the following issues or if there is a family history of any of these health issues, it may be worth doing the MTHFR test:
Taking Methotrexate: patients with a MTHFR Mutation may need lower Methotrexate doses to prevent toxicity (more on Methotrexate Toxicity below)
Depression
Insomnia
Family history of dementia
Alcoholism
Long-term use of birth control pills
Pregnant women or women wishing to become pregnant
Women with abnormal pap smears that are precancerous
Patients on dialysis
Long-term us of NSAIDS such as aspirin or ibuprofen
Personal or family history of heart disease or blood clots
Spina bifida
Preeclampsia (high blood pressure during pregnancy)
Though there is more and more research on the significance of the MTHFR Mutation, many insurances do not cover this test.
MTHFR Mutationt test looks for two types of genetic mutations:
1. C677T
2. A1298C
These mutations affect the MTHFR enzyme involved in folate metabolism in the body. Proper MTHFR enzyme function ensures that homocysteine (toxic metabolite) is properly metabolized to the amino acid methionine which then makes SAMe. SAMe is known as the “universal methyl donor” which is extremely important for serotonin, melatonin and your DNA.
Folate is a B-vitamin and is important because it is at the heart of metabolism and the production of all your cells. Without it, nothing really works well so our list of symptoms and health problems would look pretty crazy.
Who has this mutation?
Approximately 5-14% of the US population has two copies of the MTHFR mutation. It is the most common in those of Mediterranean descent and lowest in those of African ancestry.
Why is homocysteine a problem?
Some studies have shown that an elevated homocysteine levels may damage blood vessel walls leading to plaque (atherosclerosis) development and thus the potential for a heart attack, stroke or blood clot and overall cardiovascular disease, though some studies have not shown this: thus a controversy.
Homocysteine requires healthy levels of folate, vitamin B12 and vitamin B6 to be metabolized properly. Recent data however shows that supplementation with these vitamins to lower homocysteine levels does not produce any benefit regarding cardiovascular risk reduction.
What do my MTHFR test results mean?
The MTHFR test will tell you if you have two copies of the C677T variant, or one copy of the C677T and one copy of the A1298C then your MTHFR enzyme activity may be compromised. Not everyone who has these gene mutations will develop elevated homocysteine levels or health problems that are related to an abnormal MTFHR test.
What is the best form of folate?
Folic acid is actually a synthetic compound that does not occur in nature compared to folate which is found in nature and your body. Some people have difficulty metabolizing folic acid to it’s natural form in the body which results in a build-up of folic acid. This can be a problem because excessive folic acid levels have been linked to increased risk of cancer.
Folic acid is found in most commercial vitamin supplements and fortified food products. You should only take supplements that use the natural form of folate or if you have the MTHFR defect then L-5-MTHF may be best for you. The advantage of the L-5-MTHF form of folate is that it is already activated so it is ready to go whether you have the MTHFR defect or not.
How much should you take?
If you are using a high-quality supplement company then all of their products will use either natural forms of folate or the L-5-MTHF form of folate. Most products that are specific for the MTHFR mutation have either 1,000mcg or 5,000mcg of L-5-MTHF per capsule. Consult with your doctor about how much you should take or if you need it at all.
The optic neuropathy has been linked to folate deficiency, either nutritional or genetic.
Other Toxicities:
9. worsening of nodulosis,
10. pneumonitis,
11. neurologic toxicity,
12. gastrointestinal complications including nausea, vomiting and diarrhea,
13. transaminitis,
14. hematologic abnormalities,
15. rash,
16. stomatitis,
17. alopecia
Studies have showed an increased risk (or odds ratio=OR) of Methotrexate toxicity used to treat Rheumatoid Arthritis associated with the C677T polymorphism. There was no association between the A1298C polymorphism and toxicity.
Folate supplementation when co-administered with methotrexate, minimizes its adverse effectsand may therefore prevent the development of optic neuropathy. In addition, when this condition is recognized, the nerve damage can be reversed if methotrexate is stopped and appropriate folate supplementation is administered promptly.
A case was reported by Ponjavic et al. in which they described a reduced full-field ERG in b-wave amplitude in a 13-year-old boy treated with methotrexate for 8.5 years. Three years after cessation of therapy the multi-focal (mf)ERG demonstrated normal responses in the macular region.
In conclusion, as pharmacogenetics evolves more and larger studies are needed to assess the role of various polymorphisms for drug efficacy and toxicity. However, until larger studies are carried out meta-analysis of pooled data is the best available tool to validate genetic associations with efficacy and toxicity. The results presented here illustrate both the paucity of reliable pharmacogenetic data on a very commonly used anti-rheumatic drug as well as the potential role that pharmacogenetics can play in tailoring drug therapy for an individual patient.
The methylenetetrahydrofolate reductase (MTHFR) mutation test is used to detect two relatively common mutations in the MTHFRgene that are associated with elevated levels of homocysteine in the blood. It is not routinely ordered.
This test is sometimes ordered as a follow-up to an elevated homocysteine test and may be occasionally ordered along with other cardiac risk tests if a person has a personal or family history of premature cardiovascular disease (CVD) or inappropriate blood clots (thrombosis). However, its utility for assessing risk of CVD has not been established and some expert guidelines do not recommended it for thrombosis screening.
It may be ordered if a person has a close relative with known MTHFR genetic mutations, particularly if that person also has elevated homocysteine levels. MTHFR C677T and A1298C gene mutations are the most common and the ones that are typically tested. If someone has a different mutation in their family, then that specific mutation should be tested.
An MTHFR test may sometimes be ordered along with other inherited clotting risk tests, such as Factor V Leiden or prothrombin 20210 mutation tests to help evaluate a person’s overall risk of developing inappropriate blood clots.
Although the MTHFR mutation test may be used to help determine the cause of elevated homocysteine, the value of measuring homocysteine levels is not clear. While evidence from some studies suggests that elevated homocysteine levels contribute to the risk of CVD and/or thrombosis, a direct link has not been established. Routine testing for homocysteine levels as a cardiac risk marker is not recommended by the American Heart Association. The College of American Pathologists and the American College of Medical Genetics recommend against testing for the C677T variant, citing limited utility for patients with blood clots. Furthermore, use of homocysteine levels for the purpose of determining risk of CVD, peripheral vascular disease, and stroke is in doubt at this time given that several studies show no benefit or risk reduction in people who were treated with folic acid and vitamin B supplements that lowered their homocysteine level.
The MTHFR mutation test may sometimes be ordered when a person has elevated homocysteine levels, especially when the person has a personal or family history of premature cardiovascular disease or thrombosis. It may sometimes be ordered when a close relative has MTHFR gene mutations, although it may not be useful if that relative has normal homocysteine levels, and some laboratories and organizations recommend against using it for thrombophilia screening.
Results typically are reported as negative or positive and, if positive, the report will name the mutation(s) present. Often, an interpretation of the results is also provided.
Only a small percentage of cases of elevated homocysteine are due to an inherited cause. Of these, MTHFR C677T and A1298C mutations are among the most common.
If a person has two copies (homozygous) of MTHFR C677T, or has one copy of C677T and one of A1298C, then it is likely that elevated homocysteine levels are due to these inherited mutations, or that the mutations are contributing to them.
Two copies of A1298C are not typically associated with increased homocysteine levels.
If the MTHFR mutation test is negative, then the C677T and A1298C mutations were not detected and the tested person’s elevated homocysteine level is likely due to another cause. Other, more rare MTHFR genetic mutations will not be detected with typical testing.
Those with MTHFR mutations and other clotting risk factors, such as Factor V Leiden or PT 20210 mutations, may be at an increased risk of thrombosis.
People who have elevated homocysteine levels may be at an increased risk of developing premature cardiovascular disease (CVD) and/or thrombosis, but many, including those with MTHFRmutations, will never develop CVD or thrombosis. The role of homocysteine in cardiac risk assessment is still in the process of being determined.
Besides MTHFR mutations, there are other causes of elevated homocysteine levels, including deficiency of vitamins B6, B12, and/or folate; these vitamins are required for homocysteine metabolism. The MTHFR mutation may not be present with these acquired, as opposed to inherited, causes of elevated homcysteine. Additionally, if a more rare mutation of MTHFR is causing elevated homocysteine levels, the C677T and A1298C tests will not detect those other mutations.
For MTHFR mutations, the C677T variant results in substitution of the amino acid alanine for valine. The A1298C variant results in an alanine substitution (versus a gultamine). The C677T valine substitution results in a less active form of the MTHFR enzyme.
Some studies have shown links between MTHFR genetic mutations and an increased risk of neural tube defects, pre-eclampsia, and certain cancers, but the test is not used clinically with these conditions.
The MTHFR enzyme is involved in folate metabolism. Because of this, those who have MTHFR mutations and take drugs that affect folate metabolism, such as methotrexate, may be more likely to experience toxicity. An MTHFR mutation test may be performed for a person who is prescribed methotrexate in order to adjust dosages and reduce risk of toxicity.
Association Between MTHFR C677T Polymorphism and Methotrexate Treatment Outcome in Rheumatoid Arthritis Patients: A Systematic Review and Meta-Analysis.
Methotrexate (MTX) is one of the most widely used disease-modifying antirheumatic drugs for the treatment of rheumatoid arthritis (RA). However, its efficacy in RA patients is variable and unpredictable. Methylene tetrahydrofolate reductase (MTHFR) is an important enzyme in the MTX pathway and is involved in folate metabolism and DNA synthesis. Several studies have examined the association between the MTHFR C677T polymorphism and MTX toxicity and efficacy in RA, but their conclusions remain controversial.
MATERIALS AND METHODS:
We conducted a comprehensive literature search of PubMed, Embase, and Cochrane Library databases to identify studies reporting an association between the MTHFR C677T single nucleotide polymorphism and MTX response in RA patients.
RESULTS:
We identified 16 studies reporting MTX efficacy in 2373 RA cases, and 25 studies reporting MTX toxicity in 4063 RA cases. The pooled data analysis indicated that the MTHFR C677T polymorphism was associated with increased toxicity, but not efficacy, of MTX in RA patients. Further stratification based on ethnicity revealed an association between the MTHFR 677TT genotype and overall MTX toxicity in East Asian and Caucasian patient populations. In addition, RA patients with the MTHFR C677T polymorphism who were supplemented with folic acid displayed significantly elevated risk for MTX toxicity.
CONCLUSION:
Our study indicated that the MTHFR C677T polymorphism could be used as a predictor of MTX toxicity in RA patients. However, large randomized prospective studies will be required to effectively replicate and validate these findings.
References:
These are the last 200 references of MTHFR on Pubmed today.
Botticelli A, Onesti CE, Strigari L, Occhipinti M, Di Pietro FR, Cerbelli B, Petremolo A, Anselmi E, Macrini S, Roberto M, Falcone R, Lionetto L, Borro M, Milano A, Gentile G, Simmaco M, Marchetti P, Mazzuca F.
Anticancer Drugs. 2017 Mar 14. doi: 10.1097/CAD.0000000000000492. [Epub ahead of print]
Dawood RM, Mahmoud EM, Ibrahim MK, Din NG, Aboul-Enein A, Zayed N, Abd YS, Eldeen HG, Eletreby R, Elsharkawy M, Omran M, El-Shenawy R, Fayed SA, Awady MK.
Clin Lab. 2017 Mar 1;63(3):419-426. doi: 10.7754/Clin.Lab.2016.160624.
Xu B, Kong X, Xu R, Song Y, Liu L, Zhou Z, Gu R, Shi X, Zhao M, Huang X, He M, Fu J, Cai Y, Li P, Cheng X, Wu C, Chen F, Zhang Y, Tang G, Qin X, Wang B, Xue H, Chen Y, Tian Y, Sun N, Cui Y, Hou FF, Li J, Huo Y.
Medicine (Baltimore). 2017 Feb;96(8):e5862. doi: 10.1097/MD.0000000000005862.
da Silva DG, Belini Junior E, de Souza Torres L, Okumura JV, Marcel Barberino W, Garcia de Oliveira R, Urbinatti Teixeira V, Lopes de Castro Lobo C, Alves de Almeida E, Bonini-Domingos CR.
Reuter MS, Tawamie H, Buchert R, Hosny Gebril O, Froukh T, Thiel C, Uebe S, Ekici AB, Krumbiegel M, Zweier C, Hoyer J, Eberlein K, Bauer J, Scheller U, Strom TM, Hoffjan S, Abdelraouf ER, Meguid NA, Abboud A, Al Khateeb MA, Fakher M, Hamdan S, Ismael A, Muhammad S, Abdallah E, Sticht H, Wieczorek D, Reis A, Abou Jamra R.
JAMA Psychiatry. 2017 Mar 1;74(3):293-299. doi: 10.1001/jamapsychiatry.2016.3798.
Cięszczyk P, Zarębska A, Jastrzębski Z, Sawczyn M, Kozakiewicz-Drobnik I, Leońska-Duniec A, Kaczmarczyk M, Maciejewska-Skrendo A, Żmijewski P, Trybek G, Smółka W, Pilch J, Leźnicka K, Lulińska-Kuklik E, Sawczuk M, Massidda M.
J Hum Kinet. 2016 Dec 15;54:43-53. doi: 10.1515/hukin-2016-0055. eCollection 2016 Dec 1.
Moruzzi S, Udali S, Ruzzenente A, Guglielmi A, Guarini P, Martinelli N, Conci S, Mazzi F, Pattini P, Tammen SA, Olivieri O, Pizzolo F, Choi SW, Friso S.
PLoS One. 2016 Dec 9;11(12):e0167534. doi: 10.1371/journal.pone.0167534. eCollection 2016.
Huemer M, Diodato D, Schwahn B, Schiff M, Bandeira A, Benoist JF, Burlina A, Cerone R, Couce ML, Garcia-Cazorla A, la Marca G, Pasquini E, Vilarinho L, Weisfeld-Adams JD, Kožich V, Blom H, Baumgartner MR, Dionisi-Vici C.
Roberto M, Romiti A, Botticelli A, Mazzuca F, Lionetto L, Gentile G, Paris I, Falcone R, Bassanelli M, Di Pietro FR, Onesti CE, Anselmi E, Macrini S, Simmaco M, Marchetti P.
Onesti CE, Botticelli A, La Torre M, Borro M, Gentile G, Romiti A, Lionetto L, Petremolo A, Occhipinti M, Roberto M, Falcone R, Simmaco M, Marchetti P, Mazzuca F.
Danjou F, Fozza C, Zoledziewska M, Mulas A, Corda G, Contini S, Dore F, Galleu A, Di Tucci AA, Caocci G, Gaviano E, Latte G, Gabbas A, Casula P, Delogu LG, La Nasa G, Angelucci E, Cucca F, Longinotti M.
Botticelli A, Borro M, Onesti CE, Strigari L, Gentile G, Cerbelli B, Romiti A, Occhipinti M, Sebastiani C, Lionetto L, Marchetti L, Simmaco M, Marchetti P, Mazzuca F.
Dreussi E, Cecchin E, Polesel J, Canzonieri V, Agostini M, Boso C, Belluco C, Buonadonna A, Lonardi S, Bergamo F, Gagno S, De Mattia E, Pucciarelli S, De Paoli A, Toffoli G.
Giuffrè M, Verso CL, Serra G, Moceri G, Cimador M, Corsello G; Study Group of Neonatal Infectious Diseases Affiliated to the Italian Society of Neonatology..