I had never heard of anyone ingesting “Neil Smith oil.” I had no idea what my patient was talking about, when she said that she bought “Neil Smith Oil” in Maryland–apparently, it is Cannabidiol oil (Reference 3), she took it as she was having chronic pain.
What happened next was very scary and she says she would never take it again. The room started spinning, she almost passed out and could barely make it to her bed before she passed out. She wasn’t even able to call 911 until after she woke up.
I do not know how many case reports there are on the safety of CBD oil, but for now, I would not recommend trying it.
Some patients have used CBD oil or marijuana as a way of decreasing eye pressure. This is also not recommended. A recent study by Miller et.al, showed that CBD can increase intraocular pressure (Reference 1) (particularly if you are a male rat). Also the American Academy of Ophthalmology does not recommend using Marijuana (Reference 2).
Recently I had a male patient come in with the following:
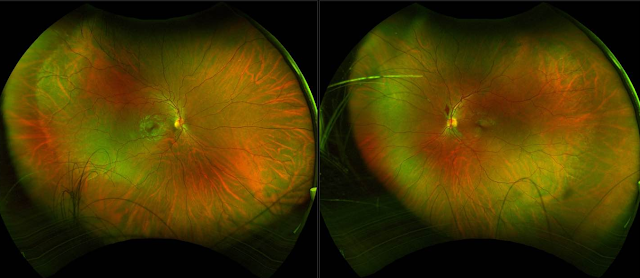
We still wonder if the new flame hemorrhage in the retina is from the marijuana or not.
He had no recent trauma, coughing, etc.
Unusual case of “excessive marijuana” (pt’s own words) use possibly leading to a flame hemorrhage in the left eye in a young 26yo male. He has very narrow angles ((ACV 76)) and discs at risk. Marijuana likely increased his eye pressure and led to this early sign of a vein occlusion. Has anyone seen this before? Blood work was negative per pt in recent past but repeating. No hx of DM, HTN, etc

SLC
PS: I did find this point interesting: that the diurnal variation of one’s pressure can be sex-dependent.
Our results also raise the possibility that the diurnal variation of IOP, in which GPR18 plays a role,35 is sex-dependent.
Abstract
Purpose: It has been known for nearly 50 years that cannabis and the psychoactive constituent Δ9-tetrahydrocannabinol (THC) reduce intraocular pressure (IOP). Elevated IOP remains the chief hallmark and therapeutic target for glaucoma, a major cause of blindness. THC likely acts via one of the known cannabinoid-related receptors (CB1, CB2, GPR18, GPR119, GPR55) but this has never been determined explicitly. Cannabidiol (CBD) is a second major constituent of cannabis that has been found to be without effect on IOP in most studies.
Methods: Effects of topically applied THC and CBD were tested in living mice by using tonometry and measurements of mRNA levels. In addition the lipidomic consequences of CBD treatment were tested by using lipid analysis.
Results: We now report that a single topical application of THC lowered IOP substantially (∼28%) for 8 hours in male mice. This effect is due to combined activation of CB1 and GPR18 receptors each of which has been shown to lower ocular pressure when activated. We also found that the effect was sex-dependent, being stronger in male mice, and that mRNA levels of CB1 and GPR18 were higher in males. Far from inactive, CBD was found to have two opposing effects on ocular pressure, one of which involved antagonism of tonic signaling. CBD prevents THC from lowering ocular pressure.
Conclusions: We conclude that THC lowers IOP by activating two receptors—CB1and GPR18—but in a sex-dependent manner. CBD, contrary to expectation, has two opposing effects on IOP and can interfere with the effects of THC.
Cannabis has a long and storied history tracing back thousands of years. Only recently have we begun to understand how its constituents act in the body. Δ9-tetrahydrocannabinol (Δ9-THC, THC) is understood to be the chief psychoactive ingredient of cannabis.1 The year 1971 marked the publication of the first work by Hepler and Frank2 demonstrating that cannabis inhalation has a salutary effect on intraocular pressure (IOP). This set in motion a flurry of research to learn the nature of this effect. Remarkably, however, we still do not know through which receptors the principal components of cannabis regulate IOP. It is often assumed that THC does this via cannabinoid CB1 receptors, since CB1 receptor agonists lower IOP3 but this has not been demonstrated. Ocular research into the two principal phytocannabinoids—THC and the noneuphoric cannabidiol (CBD)—largely ceased after the early 1980s, well before the first cannabinoid receptor was identified in 1990.4CB1 receptors remain the best-characterized cannabinoid receptor and are widely distributed in the brain5 and eye6 and regulate important physiological systems such as pain, mood, movement, and memory (for review see Ref. 7). But the cannabinoid signaling system consists not only of CB1 receptors but also of CB2,8 GPR18,9 and GPR11910 and perhaps others, as well as enzymes that produce and metabolize the lipid cannabinoid messengers (for review see Refs. 11 and 12).
THC is not the only phytocannabinoid found in cannabis: CBD can be present at quantities comparable to THC and plant strains have now been developed (e.g., Charlotte’s Web) that have a CBD to THC ratio that is heavily skewed toward CBD. Long considered inactive, CBD has shown benefit in clinical trials as an antiepileptic in Dravet’s syndrome18 and has recently been approved by the US Food and Drug Administration (FDA) as an antiepileptic. But CBD is also assigned many other properties, including activity at GPR1819,20 and the cannabinoid-metabolizing enzyme FAAH (fatty acid amide hydrolase),21 but CBD may act as a negative allosteric modulator of CB1 signaling.22,23 This is significant because this means that CBD may antagonize THC signaling. Three of four studies that have tested CBD for effects on IOP have reported no effect, but the fourth has reported an increase in IOP.24
The current study was an examination of the receptor dependence of the actions of THC and CBD on IOP.
Methods
Animals
Experiments were conducted at the Indiana University campus. All mice used for IOP experiments were handled according to the guidelines of the Indiana University animal care committee and in accordance with the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. Mice (male and female, age 3–8 months) were kept on a 12-hour (6:00 AM–6:00 PM) light/dark cycle, and fed ad libitum. Male and female mice were used for these experiments as noted and were obtained from the colony of Ken Mackie (Indiana University, Bloomington, IN, USA). Mice were C57BL/6J (C57) strain except CB1−/−mice, which were on a CD1 strain background. We have previously shown that mice on a CD1 background see reductions in ocular pressure upon topical treatment with CB1 cannabinoid agonists WIN55212 and CP55940, which are absent in CB1 knockouts.14 Mice were allowed to acclimatize to the animal care facility for at least a week before their use in experiments. A total of 85 mice were used in these experiments. CB1−/− mice were kindly provided by Ken Mackie. The knockouts were global knockouts. CB1−/− animals were originally received from Catherine Ledent (Catholic University, Leuven) as heterozygotes.25
Intraocular Pressure Measurements
IOP was measured to test the effects of topically applied THC and CBD in living mice by rebound tonometry, using a Tonolab (Icare Finland Oy, Helsinki, Finland). To obtain reproducible IOP measurements, mice were anesthetized with isoflurane (3% induction). The anesthetized mouse was then placed on a platform in a prone position, where anesthesia was maintained with 2% isoflurane. Baseline IOP measurements were taken in both eyes. Measurements were initiated promptly (typically within a minute) after successful induction of anesthesia. Depth of anesthesia was assessed by paw press. A “measurement” consisted of the average value of six readings. One eye was then treated with drug (dissolved in Tocrisolve [Tocris Biosciences, Ellisville, MO, USA]), a soya-based solvent,3 5 μL final volume, applied topically), while the other eye was treated with vehicle. Mice recover rapidly from isoflurane anesthesia. After an hour the animal was again anesthetized as above. IOP was then measured in the drug-treated and vehicle-treated contralateral eye. This procedure (recovery from anesthesia, return to cage, reanesthetization, measurement of IOP) was repeated at the 4- and 8-hour time points as necessary.
IOP measurements following drug administration were analyzed by paired t-tests comparing drug-treated eyes to contralateral vehicle-treated eyes except for animals that had a time series (1, 4, and 8 hours), in which case a 2-way ANOVA with Bonferroni post hoc test was performed.
Quantitative RT-PCR
Primers for selected components of the endocannabinoid system were designed by using Primer-Blast (http://www.ncbi.nlm.nih.gov/tools/primer-blast, in the public domain) and the corresponding mouse gene. Primer sequences are as listed below:
Eyes were extracted, the lens removed, and were then immediately stored at −80°C. RNA was extracted with a Trizol reagent (Ambion, Austin, TX, USA) and genomic DNA was removed with DNase (NEB, Bethesda, MD, USA) following the manufacturer’s instructions. RT-PCR was performed by using a one-step, Sybr Green amplification process (PwrSybr; Applied Biosystems, Carlsbad, CA, USA). Quantitative PCR was performed with an Eppendorf RealPlex2 Mastercycler thermocycler (Eppendorf, Hauppauge, NT, USA).
A primer for glyceraldehyde 3-phosphate dehydrogenase was used as an internal control for each experimental condition with the threshold cycle set within the linear range (10-fold above baseline). Once the standard critical threshold (Ct) was set, the relative expression levels for genes were determined.
Lipid Extraction and LC/MS/MS Analysis and Quantification
Enucleated eyes were flash frozen in liquid nitrogen and frozen at −80°C until used for lipid analysis. Levels of ∼35 cannabinoid-related lipids as well as arachidonic acid and several prostaglandin-family metabolites were measured by liquid chromatography (LC)/mass spectrometry (MS) from whole eyes as previously described.15,26 Briefly, eyes were homogenized, centrifuged at 19,000g at 24°C for 20 minutes and supernatant was collected. Compounds were isolated by using a partial purification of the 25% organic solution. C18 solid-phase extraction columns (Agilent Technologies, Santa Clara, CA, USA) were used with an elution of 100% methanol.
Samples were placed in an autosampler and held at 24°C (Agilent 1100 series autosampler; Palo Alto, CA, USA) for LC/MS/MS analysis. Ten to 20 μL of eluents were injected for each sample, which was rapidly separated with a C18 Zorbax reversed-phase analytic column (Agilent Technologies) to scan for individual compounds. Gradient elution (200 μL/min) then was accomplished under pressure (Shimadzu 10AdVP pumps; Shimadzu Scientific Instruments, Columbia, MD, USA). The electrospray ionization was done by using an API3000 triple quadrupole mass spectrometer (Applied Biosystems/DSM Sciex; Foster City, CA, USA). A multiple reaction monitoring (MRM) setting on the LC/MS/MS was used to analyze levels of each compound. Synthetic standards were used to generate optimized MRM methods and standard curves for analysis.
Individual animals in each of the treatment groups were coded and experiments were analyzed in a blinded fashion.
Materials
Δ9-THC and CBD were obtained through the National Institutes on Drug Abuse drug supply program. O-1918 and Tocrisolve were obtained from Tocris Bioscience.
Results
THC Lowers IOP in a Sex-Dependent Manner
We found that THC when applied topically (5 mM) lowered IOP relative to the vehicle-treated contralateral eye in male mice. This resultant drop in IOP was quite pronounced at 8 hours, with a nearly 30% drop in IOP (Fig. 1A, IOP in THC [5 mM]–treated versus vehicle-treated contralateral eye in males; 1 and 4 hours: n = 7, 8 hours: n = 8; *P < 0.05 by 1-way ANOVA with Bonferroni post hoc test versus contralateral eye at corresponding time point). Strikingly however, in female mice given the same treatment there was a more modest effect at 4 hours than the corresponding time point in males and no effect at 8 hours (Fig. 1B, IOP in THC [5 mM]–treated versus vehicle-treated contralateral eye in females; 1 and 4 hours: n = 20, 8 hours: n = 8; *P < 0.05 by 1 way ANOVA with Bonferroni post hoc test versus contralateral eye at corresponding time point). The effect of THC was therefore sex-dependent.
Figure 1

THC substantially lowers IOP for at least 8 hours but in a sex-dependent manner. (A) Topically applied THC (5 mM) lowers IOP relative to contralateral vehicle-treated eye in mouse. Effect persists for 8 hours. (B) In contrast, females only see an effect of THC at 4 hours. *P < 0.05, 1-way ANOVA with Bonferroni post hoc test versus contralateral eye at corresponding time point.
THC Lowers IOP Through Combined Activation of CB1 and GPR18 Receptors
As noted in the introduction, THC lowers IOP but the mechanism by which it does this remains undetermined. A preferred hypothesis is that THC lowers IOP via CB1 receptors. We therefore tested whether the effect of THC would be absent in CB1 receptor knockout mice. Interestingly, we found that CB1 deletion only partly eliminated the effect of THC (Figs. 2A, 2B; IOP in THC [5 mM]–treated versus vehicle-treated contralateral eye in CB1 knockout (KO) males; 1 and 4 hours: n = 12; *P < 0.05 by paired t-test versus contralateral eye at corresponding time point). This suggests that CB1 also acts via a second receptor. One likely candidate for this is the GPR18 receptor since, as noted previously, GPR18 can lower IOP in mice and is activated by THC. We therefore tested whether the GPR18 antagonist O-1918 (5 mM) applied topically to CB1 knockout mice would prevent the effect of THC. We found that there was no effect at 1 or 4 hours under this condition (Figs. 2C, 2D; IOP in O1918 pretreated [5 mM topical] CB1 KOs: THC [5 mM]–treated versus vehicle-treated contralateral eye; 1 and 4 hours: n = 5; *P < 0.05 by paired t-test versus contralateral eye at corresponding time point). This argues that THC lowers IOP through a combination of CB1 and GPR18.
Figure 2

THC lowers IOP through combined activation of CB1 and GPR18 receptors. (A, B) THC treatment in CB1 KO males still results in a partial drop in IOP at 1 hour but not at 4 hours. (C, D) THC treatment in CB1 KO mice pretreated with GPR18 blocker O1918 (5 mM) does not result in a drop in IOP relative to contralateral vehicle-treated eye. *P < 0.05, paired t-test versus contralateral eye.
CBD Has Two Independent Opposing Actions on IOP
As noted above, CBD has been tested in several studies for effects on IOP. Three of those studies found no effect, while the last saw an increase in IOP. CBD has been proposed to act on a large and growing number of receptors including recent evidence that CBD is a negative allosteric modulator at CB1 receptors.23,27 When tested in our model, we found that CBD (5 mM) in male mice substantially raised IOP at 1 and 4 hours (Figs. 3A, 3B; IOP in CBD [5 mM]–treated versus vehicle-treated contralateral eye in wild type (WT) males; 1 hour: n = 13; 4 hours: n = 19; *P < 0.05 by paired t-test versus contralateral eye at corresponding time point). Female mice saw a similar rise at both time points (data not shown). Strikingly, the same experiment in CB1 knockouts resulted in a decrease in ocular pressure at 1 hour but no effect at 4 hours (Figs. 3C, 3D; IOP in CBD [5 mM]–treated versus vehicle-treated contralateral eye in CB1 KO males; 1 and 4 hours: n = 7; *P < 0.05 by paired t-test versus contralateral eye at corresponding time point). This indicates that CBD has two opposing effects on IOP. The first and dominant effect of raising IOP is likely CB1-dependent since the effect is absent in CB1 knockout mice and may be a consequence of cannabinoid receptor antagonism. We tested whether the IOP reduction was due to activity at GPR18 receptors, since GPR18 activation can lower IOP.13 CBD had no effect on IOP in animals pretreated with the GPR18 antagonist O1918 (5 mM) (Figs. 3E, 3F; IOP in O1918-pretreated animals [5 mM topical], CBD [5 mM]–treated versus vehicle-treated contralateral eye in CB1 KO males; 1 and 4 hours: n = 7; not significant (NS) by paired t-test versus contralateral eye at corresponding time point).
Figure 3

CBD has two independent opposing actions on IOP. (A, B) CBD (5 mM) raises IOP at 1 and 4 hours. (C, D) CBD treatment in CB1 knockout mice unmasks a drop in IOP at 1 hour but not at 4 hours. (E, F) Pretreatment with the GPR18 antagonist O1918 in CB1 knockouts prevents the IOP-lowering effect of CBD at 1 hour. *P < 0.05, paired t-test versus vehicle-treated contralateral eye.
CBD Interferes With the IOP-Lowering Effects of THC
If CBD is raising pressure by acting as a negative allosteric modulator at CB1, then it is possible that coapplication of CBD and THC would cancel out the salutary effects of THC. To test this we treated mice (C57Bl/6J) with combined CBD/THC (5 mM/5 mM) and found that there was no effect on IOP relative to vehicle (Fig. 4, IOP in THC and CBD [5 mM each]–treated versus vehicle-treated contralateral eye in WT males; 1 and 4 hours: n = 7; NS by paired t-test versus contralateral eye at corresponding time point).

mRNA Levels for CB1 and GPR18 Are Higher in Eyes of Male Than Female Mice
If there is a sex dependence in the effect of THC, what is the basis of that difference? Are there fewer CB1 receptors, or GPR18 receptors, or both? One way to test this is to examine the mRNA expression of these receptors in the eyes of male versus female mice. We examined mRNA expression for CB1 and GPR18 by using quantitative PCR, finding that mRNA levels of CB1 and GPR18 were lower in female mice than male mice (Fig. 5; n = 9 per condition; *P < 0.05 unpaired t-test male versus female).

Cannabinoid-Related Lipid Species Are Elevated After CBD Treatment
Though the IOP-lowering effect is blocked by a GPR18 antagonist, the action of CBD may be direct or indirect, particularly since, as noted previously, CBD has been shown to act at the endocannabinoid-metabolizing enzyme FAAH. To explore this we measured levels of ∼35 cannabinoid-related lipids as well as several prostaglandins and related lipids 1 hour after treatment with CBD. In a given animal, one eye received CBD while the contralateral eye received vehicle (N = 6). As shown in the Table, the levels of most acylethanolamines rose, though not arachidonoyl-ethanolamine (AEA), an endogenous ligand for CB1/CB2 receptors. Levels of two N-acyl-gammaaminobutyric acid (GABA) and N-acyl-taurine species were elevated. Intriguingly, levels of the GPR18 ligand N-oleoylglycine (NOGly) and the GPR119 ligand 2-oleoylglycerol were also elevated.
Discussion
Nearly half a century after reports of a salutary effect of cannabinoids on ocular pressure we still do not know the mechanism by which this occurs. Our chief findings in normotensive mice were that THC lowers pressure substantially and for at least 8 hours, through a combined action at two receptors, CB1 and GPR18. This effect was sex-dependent, with much stronger responses in male mice. CBD in contrast had two opposing actions on IOP: raising IOP in wild-type animals but lowering it in CB1 knockout mice likely via GPR18. Finally, at equal concentrations CBD prevented the IOP-lowering effects of THC.
Sex-dependent effects have been reported for cannabis (e.g., in the study by Cooper and Haney28) but sex dependence had not been explored for cannabinoid regulation of IOP. Phytocannabinoids are not currently considered a suitable first-line therapeutic for glaucoma (e.g., American Academy of Ophthalmology [AAO] position statement 2014, www.aao.org); however, this may be based on limited evidence. The central argument is that topical THC is not effective, therefore necessitating treatment via cannabis inhalation. Cannabis inhalation, in turn, has assorted shortcomings: (1) psychoactivity, (2) short action (<4 hours), and (3) elevation of blood pressure. A key question then is whether topical THC works in humans. The negative conclusion is based on four studies, three of which pool male and female subjects. In the two 1981 studies by Merritt et al.,29,30 most subjects are female (4/6, 7/8). Green and Roth31 (1982) do not specify the makeup of their subject pool but exclude pregnant subjects, implying the presence of females, leaving only one study that includes only males.32 The sex dependence of THC regulation of IOP, with the robust effects in males that we report here, combined with topical THC studies in animals (e.g., Merritt et al.,29 Green et al.,33 ElSohly et al.,34), suggests that the question of topical THC as a means to lower ocular pressure may merit some reconsideration.
It is notable that no less than three cannabinoid related receptors, namely, CB1, GPR18, and GPR119, each lower IOP when activated. Moreover, they all exhibit sex dependence, but differentially. mRNA expression of CB1 and GPR18 is elevated in male mice relative to female mice. It must be noted that differential mRNA expression does not necessarily correspond to protein levels (e.g., Western blot). However the difference in mRNA is consistent with our finding that dual activation of these receptors by THC yields a stronger effect in males. In contrast, the X-linked GPR119 receptor lowers IOP preferentially in female mice.15 Our results also raise the possibility that the diurnal variation of IOP, in which GPR18 plays a role,35 is sex-dependent.
The elevation of IOP by CBD is consistent with CB1 antagonism. If CBD truly interferes with the actions of THC then low-CBD strains may offer superior results for studies involving cannabis inhalation. The second mechanism of action for CBD—the one that underlies IOP—reduction—may be due to direct or indirect activity at GPR18, since there is no effect on IOP by CBD if GPR18 and CB1 are both blocked/deleted. As noted above, CBD has been shown to be active at GPR1819,20 and may block FAAH,21 which could also elevate acylethanolamines, as we have recently shown,35 including AEA, a precursor for GPR18 ligand NAGly.9 Our lipidomic analysis revealed rises in several cannabinoid-related lipids. Levels of GPR18 ligand NAGly were not elevated but we did see a rise in the closely related NOGly, which may also activate GPR18 (data not shown). This may account for the observed GPR18-dependent effects. Levels of four of the six acylethanolamines tested were seen to rise after CBD treatment. Interestingly, of these, oleoylethanolamide (OEA) and palmitoylethanolamide have been shown by Syed et al.36 to activate GPR119, which can also lower ocular pressure in female—but not male—mice when activated.15 Moreover, levels of 2-oleoylglycerol, a GPR119 ligand that also lowers IOP,15 were also seen to rise and may contribute to the signaling profile of CBD.
One consideration in interpreting the duration of effects of THC and CBD relates to rates of metabolism and clearance. We did not assess the pharmacokinetics of these compounds. Since they are structurally quite similar (with identical molecular weight), it is unlikely that one of the original compounds is removed much more rapidly than the other. However, while the hepatic metabolism of these compounds has been studied extensively, potential metabolism in the eye is unstudied. In principle, the apparent temporal difference between CBD and THC effects in the eye may be a function of differential ocular metabolism. In principle CBD and THC may also impact each other’s metabolism, the so-called entourage effect. Competition for enzymatic breakdown is generally hypothesized to enhance the signaling of THC, whereas we saw a diminished response, but it is difficult to ascertain without further, explicit study of THC/CBD pharmacokinetics in the eye.
It is valuable to understand the mechanisms by which THC and CBD regulate intraocular pressure, particularly at a time when their changing legal status and the perception of phytocannabinoids as safe contribute to a continued growth in their availability and popular embrace. CBD in particular has recently been approved by the FDA as an antiepileptic and is available in many grocery stores. We find that the regulation of ocular pressure by THC and CBD is more complex than previously appreciated. THC acts via a combination of CB1 and GPR18 receptors in a sex-dependent manner, while CBD can both raise IOP and interfere with the effects of THC. The potential of CBD to elevate ocular pressure should be evaluated further as a potential deleterious side effect, particularly with long-term use. Our finding of sex dependence of cannabinoid regulation of ocular pressure suggests that the current academic view that topical phytocannabinoids are without effect (e.g., the 2014 AAO position statement on cannabis and glaucoma) may be premature. Most of the studies on which this position is based include female subjects but are underpowered to evaluate a potential sex dependence of effect. However, it should be stressed that the findings presented here highlight the complex endogenous cannabinoid signaling system that can be selectively targeted and harnessed to lower ocular pressure by other means. For instance, we have shown that it is possible to enhance endogenous cannabinoid signaling by blocking the cannabinoid-metabolizing enzyme monoacylglycerol lipase37 and so lower ocular pressure. Similarly, we have found that activating CB1 directly38 can achieve the same outcome. Our findings for THC suggest that a dual CB1/GPR18 agonist may prove advantageous. The study of phytocannabinoids such as THC and CBD, but also others derived from the plant, may therefore point to novel strategies to promote ocular health.
Acknowledgments
Supported by a grant from the National Institutes of Health (EY024625).
Disclosure: S. Miller, None; L. Daily, None; E. Leishman, None; H. Bradshaw, None; A. Straiker, None
References
Reference 2
AAO Does not recommend Marijuana to treat Glaucoma.
Does Marijuana Help Treat Glaucoma or Other Eye Conditions?
Cannabis and currently available compounds derived from marijuana – like CBD – are not an adequate treatment for glaucoma, or any eye condition. To treat glaucoma, eye pressure must be managed 24 hours a day. Marijuana is not a practical treatment for constant use. And more research is still needed into the exact effects of cannabis and cannabis compounds on eye pressure and glaucoma.
The American Academy of Ophthalmology does not recommend marijuana or other cannabis products for the treatment of glaucoma. The American Glaucoma Society and the Canadian Ophthalmological Society agree.
Several current, effective treatments for glaucoma are more reliable and safer than marijuana. If you have glaucoma, you should follow your ophthalmologist’s advice to get the treatment that’s right for you.
The bottom line about marijuana and glaucoma is:
- The largest association of eye physicians and surgeons in the world does not endorse cannabis or its derivatives as a glaucoma treatment.
- Do not self-medicate with marijuana in an attempt to treat glaucoma. You can lose your vision if you don’t have a reliable, effective treatment for glaucoma.
- Speak with your ophthalmologist to find the glaucoma treatment option that’s best for you.
- Tell your doctor if you do use marijuana regularly.
What is the Connection Between Glaucoma and Marijuana?
Glaucoma is an eye condition in which the optic nerve becomes damaged over time, first reducing peripheral vision before possibly leading to total blindness. One cause of optic nerve damage in glaucoma is higher-than-normal eye pressure (intraocular pressure or IOP).
As marijuana has been legalized for medical or recreational use in more U.S. states and Canada, it has become more visible and discussed as a possible treatment for many health conditions. Research in the 1970s and 1980s did show a measurable decrease in intraocular pressure for three or four hours after smoking cannabis or ingesting THC as a pill or injection. But to treat glaucoma and save vision, eye pressure has to be controlled 24 hours a day.
To reduce intraocular pressure by 3 to 5 mm Hg — and maintain that reduction — you would have to ingest about 18 to 20 mg of THC six to eight times a day, every day. The possible negative effects on mood, mental clarity and (if smoked) lung health would be significant. You would not be able to drive, operate machinery or engage in many common activities. In addition, the cost of using marijuana every three to four hours, every day makes it cost-prohibitive for most patients.
As a comparison, alcohol also has a moderate intraocular pressure-lowering effect for an hour or so after a drink. But no doctor would recommend that you drink alcohol every hour to treat glaucoma. Many other effective treatments are available that don’t have the side-effects of alcohol.
Studies Haven’t Proven That THC is Effective or Reliable for Glaucoma Treatment
Studies have been done on THC eye drops, pills and cigarettes. Eye drops led to burning, irritated eyes and were shown to not lower eye pressure. A sublingual (placed in the mouth under the tongue) THC compound found no reduction in intraocular pressure. For another study, glaucoma patients were offered THC-containing pills and/or cigarettes. Within nine months all of them asked to stop due to side effects.
As scientists learn more about glaucoma, they have also come to understand that high intraocular pressure in the fluid at the front of the eye is not the only cause of optic nerve damage. Increasing evidence shows that reduced flow of blood to the optic nerve may also cause damage in patients with glaucoma. Marijuana not only lowers eye pressure, it also lowers blood pressure throughout the body. As a result, marijuana has the potential to lower the blood flow to the optic nerve, effectively canceling out the benefit of lowered intraocular pressure.
What About CBD for Glaucoma?
In recent years, CBD has received a lot of attention and scrutiny. CBD is a derivative of cannabis that doesn’t have mood-altering effects. But just like cannabis that’s smoked or eaten, there is no accepted, current research that shows CBD to be an effective treatment for glaucoma. In fact, one recent study showed that CBD may actually increase IOP, which would make glaucoma worse.
What is the Future of Marijuana for Glaucoma Treatment?
Currently, the only way to control glaucoma and prevent vision loss is to lower the pressure in your eye. Your ophthalmologist can treat glaucoma with medication, such as prescription eye drops, or surgery, depending on the type of glaucoma and how severe it is.
Scientists are exploring whether the active ingredients in marijuana may yet offer a glaucoma treatment. If the effects of cannabis compounds can be isolated, made to be long-acting, and the side effects eliminated, they may lead to new treatments in the future. However, such developments require more research and are years away from becoming a reality.
Ref 3
CBD oil being sold in Lincoln
By Ellis Wiltsey |
Posted: Fri 10:53 PM, Nov 16, 2018






Cannabidiol or CBD oil is a hot topic nationally as of late. It’s commonly used for pain relief and for the most part is illegal in Nebraska, but many including a former Husker great use it for medicinal purposes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neil Smith is most known for his work on the football field, at both Nebraska and then in the NFL. These days, he struggles with chronic pain, which he says CBD oil helps relieve almost instantly. The Attorney General and the Nebraska Legislature still say that CBD in that capacity, is illegal.
“Medical marijuana comes from the cannabis plant,” says Jamie Woolard of CBD American Shaman “our product comes from the hemp plant. The cannabis plant contains a high level of THC, which very simply is what makes people high”
CBD American Shaman recently opened its first store in Lincoln near 23rd Street and Cornhusker Highway. It carries over 125 different products that contain the oil. Neil Smith is a spokesperson for the brand and uses the products in his everyday life.
“I don’t have the aching headaches no more,” said Smith “I’ve started sleeping a little better at night. The main objective is that my pain level is really really gotten under control and I can say that I am pain free”
CBD in any capacity, other than products obtained and approved by a UNMC study or in a drug product approved by the FDA, remain illegal in Nebraska. The Attorney General re-issued a statement today of the law which said “Cannabidiol has been and continues to be included in Nebraska’s Uniform Controlled Substances Act’s legal definition of ‘marijuana'”
CBD American Shaman says it does not believe what they’re doing is illegal.
“I would say read the last line in the statement that was put out today,” said Woolard “apparently they charged someone with selling a CBD product and it says in the last line the court threw it out because they didn’t have enough evidence to prove it was a drug, this is not a drug”
The store also says they hope to open up the conversation about CBD oil.
“This is changing people’s lives,” said Smith “and when I say changing people’s lives in a positive way we are trying to bring awareness to people that want to bring awareness to people’s bodies”
The Attorney General told law enforcement that CBD should be treated as a schedule one controlled substance and act accordingly. As for CBD American Shaman, they say despite the message their products will remain on shelves.