Central Retinal Artery Occlusion (CRAO):
Acutely
and
In Patients with a History of Strokes
Vision loss is always a medical emergency. Sudden vision loss is even more of an emergency! If a patient has a Central Retinal Artery Occlusion, which is one of the worst things one can have, there are only about 4 hours before permanent loss of vision occurs.
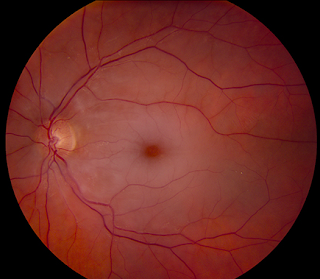
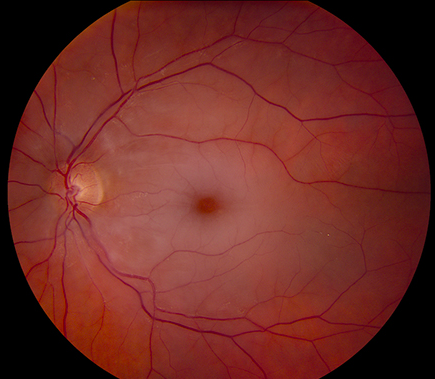
Central Retinal Artery Occlusion occurs when the central retinal artery becomes blocked, usually due to an embolus (a clot of fibrin and blood cells). It causes sudden, painless, unilateral, and usually severe vision loss.
In a CRAO: At 240 min, complete or almost total optic nerve atrophy and nerve fiber damage resulting in massive irreversible retinal damage was found in all eyes in a Hayreh study in 2004.1 This suggests that the time window for intervention is finite and inversely proportional to the degree of recovery: the longer you wait to for treatment, the less likely your vision will recover. The exact retinal tolerance time when irreversible damage occurs is not yet known, but would appear to be no longer than 4 h per Dr. Hayreh.1
There was, however, 1 case report in 2015 (from Japan) of a 78 yo man with sudden CRAO who presented within about 3 hrs of the beginning symptoms of CRAO. He was able to get cervical surgical embolectomy, 2 h and 28 min after the patient’s arrival at our hospital. He recovered his site in 4 months.
This is how they saved his vision:
1. They rushed him to Diffusion-weighted images (DWIs) magnetic resonance imaging (MRI) of the brain. When that did not show anything, the did
2. Magnetic resonance angiography (MRA) of the head & neck: this showed occlusion of the right internal/external carotid artery (ICA/ECA) and the right ophthalmic artery was not visualized. Neck MRA did not show any signal intensity of the right ICA/ECA or of the right common carotid artery (CCA). Magnetization prepared rapid gradient echo (MPRAGE) image showed loss of black signal in the right CCA with no obvious deposition of vulnerable plaque. Considering his past history of two embolic strokes attributable to chronic Af, the sudden-onset clinical course, and negative atherosclerotic arterial stenotic lesions in the MRA 10 months prior, theyw inferred that cardiogenic emboli occluded both the right ECA and ICA, which caused his total monocular visual loss due to CRAO.
3. They considered the following options:
a. IV t-PA: was considered not appropriate in their patient’s condition, since large cervical emboli could migrate further into the intracranial ICA or middle cerebral artery (MCA), causing devastating cerebral infarction.
b Emergent endovascular treatment was not available at our institution.
c. Cervical surgical embolectomy was what they did. After thorough discussion with him and his family, the operation started 2 h and 28 min after the patient’s arrival at our hospital.
In 2007, Johns Hopkins showed benefit in Local intraarterial fibrinolysis administered in aliquots in patients who presented within 15 hours of vision loss.
This is what they did:
1.Standard therapy of CRAO included ocular paracentesis, carbogen inhalation, topical intraocular pressure-lowering agents, or a combination of these. All patients eligible for LIF underwent CT or MRI with a fluid-attenuated inversion recovery sequence to exclude cerebral hemorrhage.
2. A diagnostic 4-vessel angiogram was performed under local sedation to assess the intracranial vasculature with an emphasis on the patency of the ipsilateral carotid and ophthalmic arteries.
3. LIF was performed by advancing a guide catheter using a fluoroscopic roadmap of the internal carotid artery ipsilateral to the affected eye, after which 3000 U of heparin was infused to prevent periprocedural thrombosis. A 1018 microcatheter (Boston Scientific, Natick, Mass) steamed to the shape conforming to the ophthalmic artery siphon was then advanced to the origin of the ophthalmic artery and aliquots of 3 mg tPA, in 3 cc normal saline increments, were infused over 5 minutes each. Aliquot infusion was stopped if there was a clinical VA improvement or a prespecified maximum dose of 20 mg of tPA was reached, at which time the guiding and microcatheters were removed. All patients were admitted to an intensive care unit and partial thromboplastin time was measured every 2 hours. Once the partial thromboplastin time value had dropped below 1.5 times the normal value, an infusion of intravenous heparin was begun, without a bolus, using a weight-based nomogram. Once the therapeutic range of a partial thromboplastin time value of 1.5 to 2.5 times normal was reached, the partial thromboplastin time was checked every 6 hours. The intravenous heparin infusion was stopped after 24 hours. (Reference 5)
But they note: Nevertheless, because of the nonrandomized nature of this and previous studies, LIF use cannot be recommended as standard therapy in daily clinical practice pending the publication of randomized clinical trials. Such a trial is already underway in Europe, and a further trial in North America may be warranted in light of these findings.
More Information:
Central retinal artery occlusion (CRAO) was first described by von Graefes in 1859. It is essentially an acute stroke of the eyeball–its arteries–it’s central artery. It is a true opthalmic emergency as time is of the essence: if you can get to the patient within 4 hours. If the patient had a loss of vision more than 4 hrs, then there is very unlikely there is much that can be done.
CRAO signifies end-organ ischemia (or severe loss of oxygen) and often indicates underlying atherosclerotic disease (the arteries become narrowed and hardened due to an excessive build up of cholesterol plaque around the artery wall. The disease disrupts the flow of blood around the body, posing serious cardiovascular complications.).
The incidence is estimated to be 1 in 100 000 people and accounts for 1 in 10 000 ophthalmological outpatient visits.
A prospective study of 260 eyes with CRAO showed that people suffer profound monocular visual loss, with 80% of patients having a visual acuity (VA) of 20/400 or worse. This reduction in vision increases the fall risk and thus results in increased dependency, and in worst-case scenarios leads to institutional care.
CRAO and the underlying atherosclerotic risk factors often at the root, increase the risk of future cerebral stroke and ischemic heart disease.
Although analogous to a cerebral stroke, there is currently no guideline-endorsed evidence for treatment.
Current options for therapy include the so-called ‘standard’ therapies, include the following:
1. sublingual isosorbide
2. dinitrate,
3. systemic pentoxifylline or inhalation of a carbogen,
4. hyperbaric oxygen, ocular massage, globe compression,
5. intravenous acetazolamide and mannitol,
6. anterior chamber paracentesis, and methylprednisolone.
However, none of these therapies has been shown to be better than placebo and many of them have serious risks. (Ref 2)
There has been recent interest in the use of tissue plasminogen activator (tPA) with two recent randomized controlled trials on the treatment of acute CRAO but it is hard to find a hospital that will use this as it is not covered by any insurance, is very expensive, and is still in the investigative phase.(Reference 3, 4) .
In Patients with a History of Strokes:
Treatment will depend on when the patient presents. If less than 4 hrs, the above aggressive protocols is best. If more than 24hrs, there may be little benefit & the risks may not be worth it. The patient and family with their medical team will need to decide if the benefits outweigh the risks for that particular patient, especially if the patient presents after 4 hrs. If a patient has a history of multiple strokes in the past, has a history of uncontrolled hypertension, diabetes, dialysis, etc, the risks may be too high and anti-coagulation may be the safest option to prevent a further stroke. Still an MRI, MRA, angiogram, and ECHOCARDIOGRAM should be done to assess the benefit/risk profile and prognosis of TPA, Emergency Endovascular Treatment, and Cervical Surgical Embolectomy if indicated.
References:
- Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion. Retinal survival time. Exp Eye Res. 2004;78:723–736
- Fraser SG, Adams W. Interventions for acute non-arteritic central retinal artery occlusion. Cochrane Database Syst Rev. 2009;1:CD001989. [PubMed]
- Feltgen N, Neubauer A, Jurklies B, Schmoor C, Schmidt D, Wanke J, et al. Multicenter study of the European Assessment Group for Lysis in the Eye (EAGLE) for the treatment of central retinal artery occlusion: design issues and implications. EAGLE Study report no. 1. Graefe Arch Clin Exp Ophthalmol. 2006;244:950–956. [PubMed]
- Chen CS, Lee AW, Campbell B, Lee T, Paine M, Fraser C, et al. Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion. Stroke. 2011;42:2229–2234.
-
del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA, Gent M. PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. Stroke. 1998; 29: 4–11.
-
More Information:
1.
Surg Neurol Int. 2015 Feb 18;6:29. doi: 10.4103/2152-7806.151612. eCollection 2015.
Emergent cervical surgical embolectomy to rescue total monocular blindness due to simultaneous cervical internal and external carotid artery occlusion by cardiogenic emboli.
Abstract
BACKGROUND:
Central retinal artery occlusion (CRAO) is a stroke of the retina and is associated with extremely poor prognosis. Although the pathophysiology of CRAO is diverse, including autoimmune or hematological disorders, neurosurgeons can perform carotid endarterectomy for the causal internal carotid artery stenosis or perform acute recanalization of the extra- or intracranial artery occlusion due to cardiogenic embolism.
CASE DESCRIPTION:
A 78-year-old male with a history of atrial fibrillation (Af) visited our hospital with a chief complaint of right monocular blindness. Magnetic resonance imaging revealed occlusion of the right internal and external carotid arteries. We performed emergent cervical surgical embolectomy for restoration of vision. Recanalization was accomplished within 8 h after onset, and the patient regained practical vision within 4 months.
CONCLUSION:
In the diagnosis and treatment of CRAO, occlusion of the internal and/or external carotid artery due to large cardiac emboli should be taken in consideration, especially when the patient has a history of Af, since acute recanalization might restore vision.
Abstract
Background:
Central retinal artery occlusion (CRAO) is a stroke of the retina and is associated with extremely poor prognosis. Although the pathophysiology of CRAO is diverse, including autoimmune or hematological disorders, neurosurgeons can perform carotid endarterectomy for the causal internal carotid artery stenosis or perform acute recanalization of the extra- or intracranial artery occlusion due to cardiogenic embolism.
Case Description:
A 78-year-old male with a history of atrial fibrillation (Af) visited our hospital with a chief complaint of right monocular blindness. Magnetic resonance imaging revealed occlusion of the right internal and external carotid arteries. We performed emergent cervical surgical embolectomy for restoration of vision. Recanalization was accomplished within 8 h after onset, and the patient regained practical vision within 4 months.