Which Eye Implant is Best?
Still, we know these lens implants are better than what we have ever had in the history of the world. This is very exciting, but still leaves patients and surgeons trying to find the best implant for You and Your situation.
It is important for you to do your own research and do a bit of soul searching to see what are the most important things you like to do in life: do you like to do needle work, or fix watches, or play golf, or drive at night time; are you a pilot; would you be miserable if you had to live with noticing halos and glare? Are you super analytical or a type A or AAA personality?
Answering these questions and being open with your surgeon will help you and your surgeon be happy with the final result.
Even though we do live in the 21st Century and the technology to get patients back to the vision they had when they were younger is amazing and exciting, it is not 100% guarantee you will get the perfect result or be 100% happy even with 20/20 vision. The tear film, mild residual corneal astigmatism can affect the quality of your vision.
Below are some key factors that will help you decide which implant to choose.
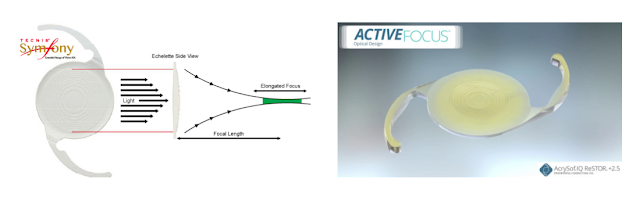
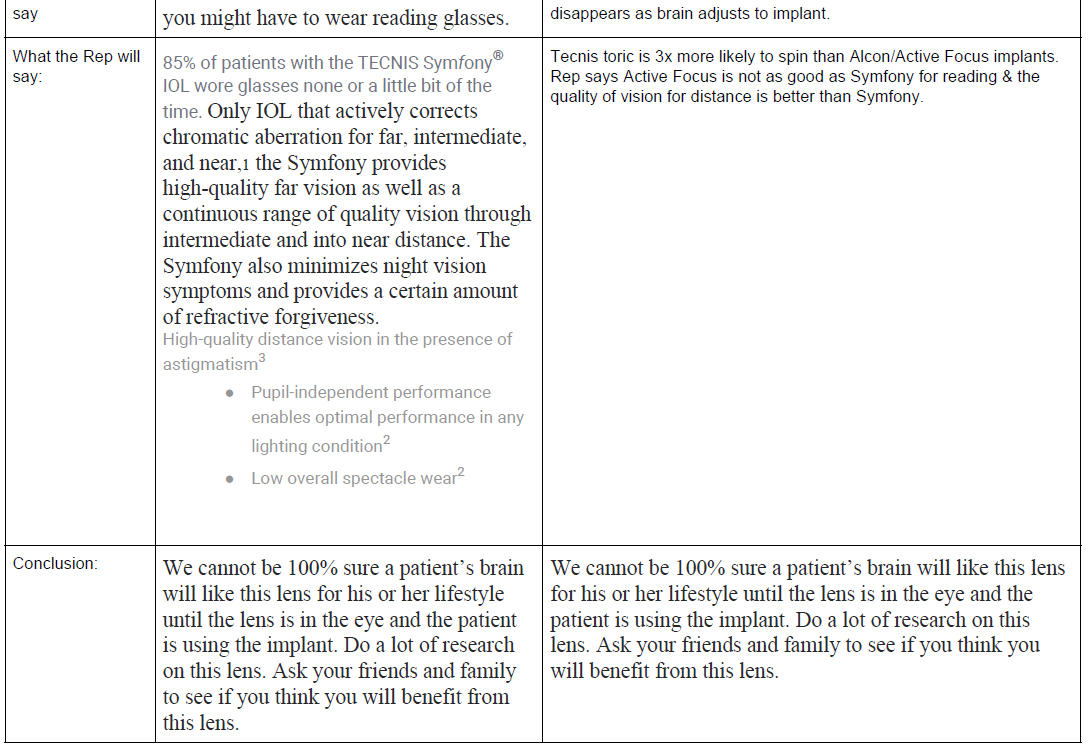
I am not paid by any of these companies so feel I can be very objective about which implants are best. I have implanted every implant available in the Advanced Technology Implant category. Personally, I feel Symfony is currently the best implant in the world. Active Focus is exciting but time will tell if this implant gives better long term results than Symfony.
Either way, if I needed cataract surgery I would
choose Femtosecond Cataract Surgery with a Symfony implant knowing I might still need reading glasses to read and may have some halos and glare when looking at lights.
Sandra Lora Cremers, MD, FACS
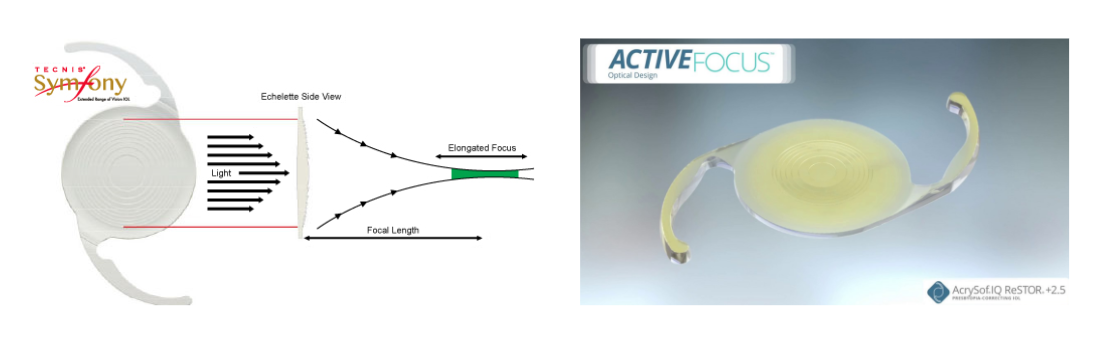

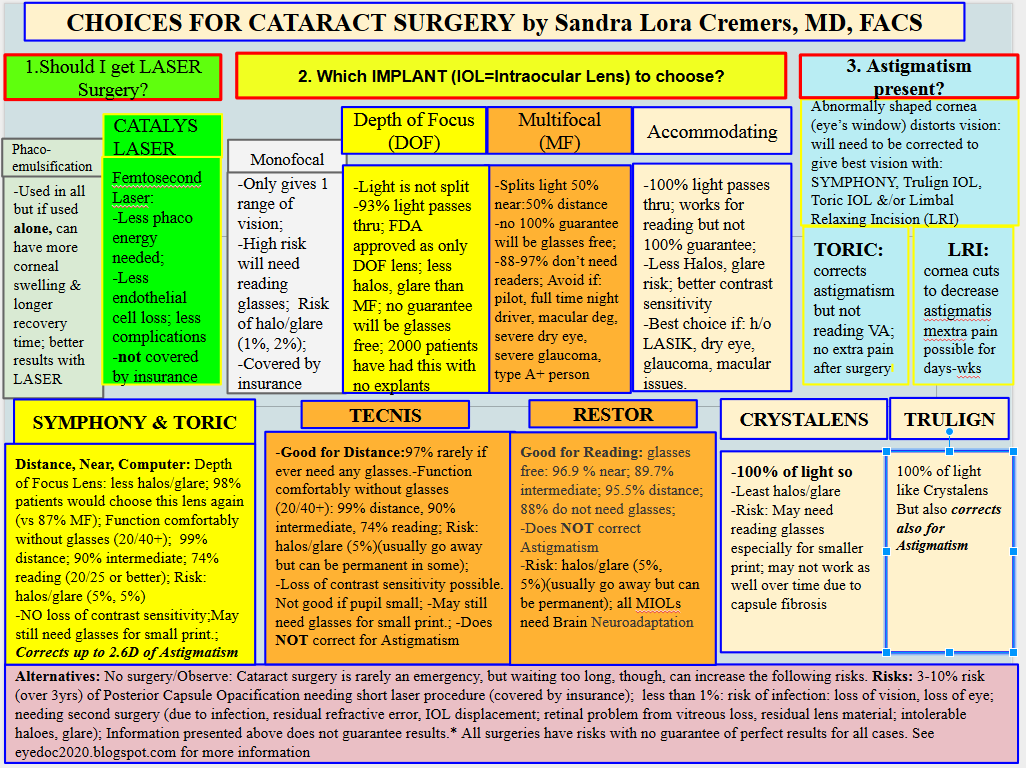
Here is a Comparison of the Usual Implant options before Active Focus came out in 2017:

More information:
https://www.accessdata.fda.gov/cdrh_docs/pdf/P980040S065C.pdf

Contraindications There are no known conditions under which the TECNIS® Symfony Extended Range of Vision IOLs should not be used.
- Reduced incidence of halos and glare compared to a traditional multifocal IOL, with a 31 patient study reporting no spontaneous complaints of glare or halos at three months after implantation of the Tecnis Symfony®.1
- Improved contrast sensitivity and reduced chromatic aberration (an effect resulting from a failure of a lens to focus all colors to the same convergence point) compared to traditional multifocal IOLs.1
- Astigmatism correction can be included in the Tecnis Symfony® IOL, removing what was once a barrier to restoring a range of focus after cataract surgery.1
WARNING: The TECNIS Symfony® IOL may
cause a reduction in contrast sensitivity under certain conditions, compared to an aspheric monofocal IOL. The physician should carefully weigh the potential risks and benefits for each patient, and should fully inform the patient of the potential for reduced contrast sensitivity before implanting the lens in patients. Special consideration of potential visual problems should be made before implanting the lens in patients with macular disease, amblyopia, corneal irregularities, or other ocular disease which may cause present or future reduction in acuity or contrast sensitivity. Patients implanted with the lens should be informed to exercise special caution when driving at night or in poor visibility conditions.
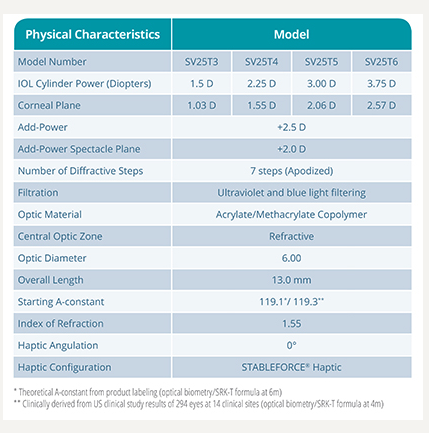
This is ACTIVEFOCUS’s IOL insert information:
Below is an Older Post: Things have changed!!
Which Eye Implant is Best?
Which Intraocular Implant is Best for Me?
It remains the best time in history to have a cataract. Cataracts are no longer the leading cause of blindness in developed areas, though it remains so in developing countries. A new intraocular lens was just approved in the US by the FDA and it has promise to improves the reading, distance, AND computer vision and total visual outcomes of all our patients.
I am not sponsored by any drug company, so below are the pros and cons of each available lens. As of October 2016, I would choose the Catalys Femtosecond Laser AND the Symfony lens for myself or any of my family members.
Sandra Lora Cremers, MD, FACS
Here is more information about the Symfony Lens.
It is a website based in Europe so the website give information on many types of implants we do not have access to in the US as they are still not FDA approved. But I love the idea of patients plugging in what they want from an implant and the best options popping up.
https://www.mylifestylelens.com/intraocular-lens/tecnis-symfony-zxr00/
Here is more information about the other types of implants other than Symfony.
http://www.aao.org/eye-health/diseases/cataracts-iol-implants
IOL Implants: Lens Replacement and Cataract Surgery
Cataract lens replacement: How IOLs work
Which lens option is right for you?
- Before surgery your eyes are measured to determine your IOL prescription, and you and your Eye M.D. will compare options to decide which IOL type is best for you, depending in part on how you feel about wearing glasses for reading and near vision.
- The type of IOL implanted will affect how you see when not wearing eyeglasses. Glasses may still be needed by some people for some activities.
- If you have astigmatism, your Eye M.D. will discuss toric IOLs and related treatment options with you.
- In certain cases, cost may be a deciding factor for you if you have the option of selecting special premium lOLs that may reduce your need for glasses.
Intraocular lens (IOL) types
- Monofocals are set to provide best corrected vision at near, intermediate or far distances.
- Most people who choose monofocals have their IOLs set for distance vision and use reading glasses for near activities. On the other hand, a person whose IOLs were set to correct near vision would need glasses to see distant objects clearly.
- Some who choose monofocals decide to have the IOL for one eye set for distance vision, and the other set for near vision, a strategy called “monovision.” The brain adapts and synthesizes the information from both eyes to provide vision at intermediate distances. Often this reduces the need for reading glasses. People who regularly use computers, PDAs or other digital devices may find this especially useful. Individuals considering monovision may be able to try this technique with contact lenses first to see how well they can adapt to monovision. Those who require crisp, detailed vision may decide monovision is not for them. People with appropriate vision prescriptions may find that monovision allows them see well at most distances with little or no need for eyeglasses.
- Presbyopia is a condition that affects everyone at some point after age 40, when the eye’s lens becomes less flexible and makes near vision more difficult, especially in low light. Since presbyopia makes it difficult to see near objects clearly, even people without cataracts need reading glasses or an equivalent form of vision correction.
These newer IOL types reduce or eliminate the need for glasses or contact lenses.
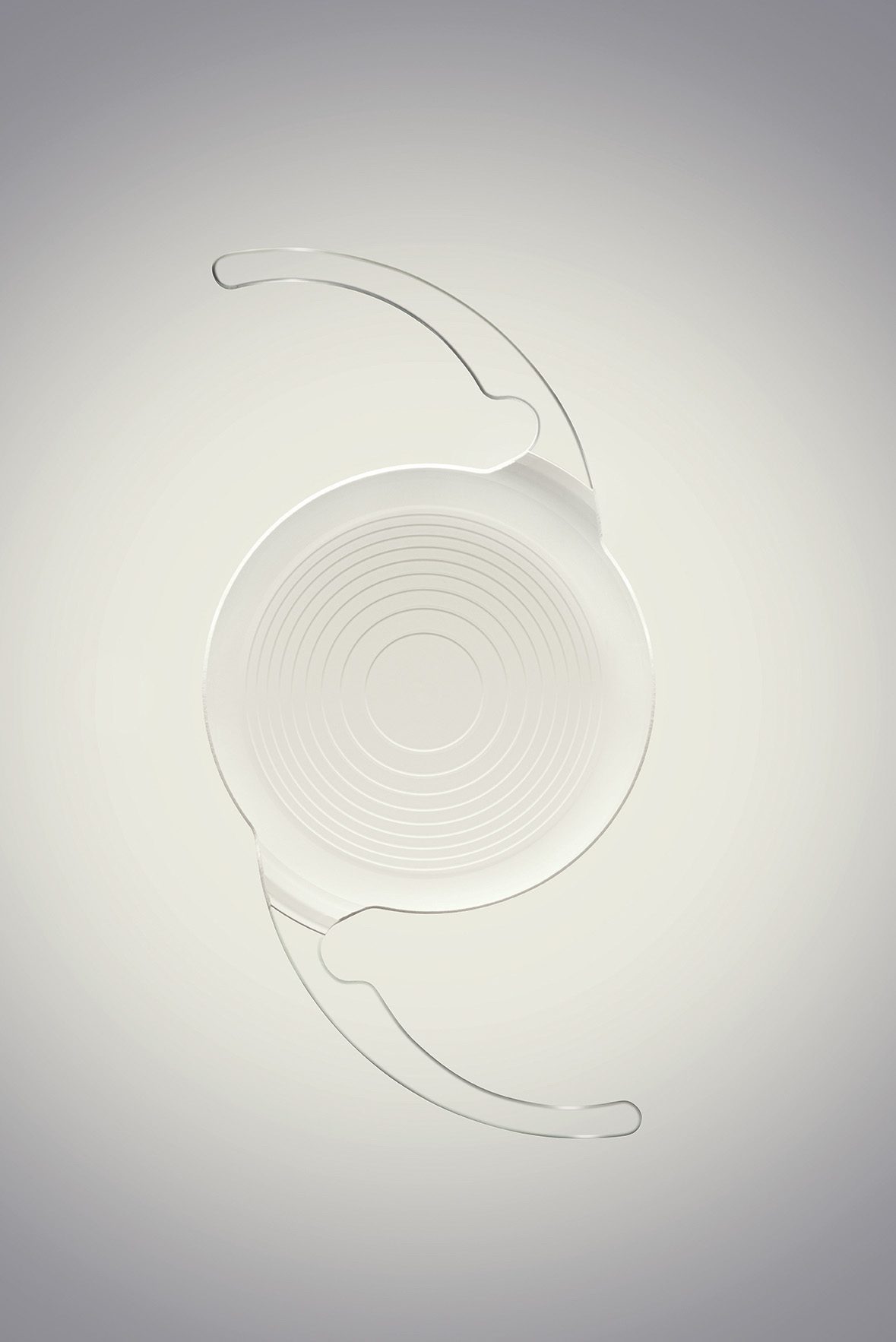
- In the multifocal type, a series of focal zones or rings is designed into the IOL. Depending on where incoming light focuses through the zones, the person may be able to see both near and distant objects clearly.
- The design of the accommodative lens allows certain eye muscles to move the IOL forward and backward, changing the focus much as it would with a natural lens, allowing near and distance vision.
- The ability to read and perform other tasks without glasses varies from person to person but is generally best when multifocal or accommodative IOLs are placed in both eyes.
- It usually takes 6 to 12 weeks after surgery on the second eye for the brain to adapt and vision improvement to be complete with either of these IOL types.
- For many people, these IOL types reduce but do not eliminate the need for glasses or contact lenses. For example, a person can read without glasses, but the words appear less clear than with glasses.
- Each person’s success with these IOLs may depend on the size of his/her pupils and other eye health factors. People with astigmatism can ask their Eye M.D. about toric IOLs and related treatments.
- Side effects such as glare or halos around lights, or decreased sharpness of vision (contrast sensitivity) may occur, especially at night or in dim light. Most people adapt to and are not bothered by these effects, but those who frequently drive at night or need to focus on close-up work may be more satisfied with monofocal IOLs.
This is a monofocal IOL with astigmatism correction built into the lens.
- Astigmatism: This eye condition distorts or blurs the ability to see both near and distant objects. With astigmatism the cornea (the clear front window of the eye) is not round and smooth (like a basketball), but instead is curved like a football. People with significant degrees of astigmatism are usually most satisfied with toric IOLs.
- People who want to reduce (or possibly eliminate) the need for eyeglasses may opt for an additional treatment called limbal relaxing incisions, which may be done at the same time as cataract surgery or separately. These small incisions allow the cornea’s shape to be rounder or more symmetrical.
Other important cataract lens replacement considerations
- In some cases, after healing completely from the cataract lens surgery, some people may need further correction to achieve the best vision possible. Their ophthalmologist may recommend additional surgery to exchange an IOL for another type, implant an additional IOL, or make limbal relaxing incisions in the cornea. Other laser refractive surgery may be recommended in some cases.
- People who have had refractive surgery such as LASIK need to be carefully evaluated before getting IOLs because the ability to calculate the correct IOL prescription (PDF 650K) may be affected by the previous refractive surgery.
Additional cataract information resources
Tecnis Symfony®
FDA Approves the Tecnis Symfony® Intraocular Lenses, the First and Only Extended Depth of Focus Lenses for People with Cataracts
- Approval includes Toric version of Symfony IOL for people with astigmatism
- Lenses provide high-quality continuous vision so patients can see clearly at near, intermediate and far-away distances, and points in between, while wearing glasses less
Media
Abbott/lens b-roll and cataract/eye animation

Symfony Lens animation

Symfony Lens


Related Links
Abbott.com
Download Abbott/lens b-roll and cataract/eye animation Download Symfony Lens animation
Related Documents
What are Cataracts?
The Ongoing Evolution of Cataract Surgery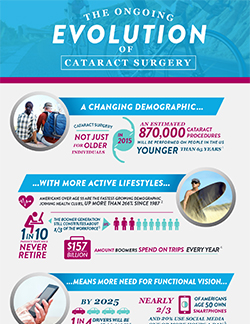
Abbott IOL Fact Sheet
Follow Us on Twitter
And Find Us On
PR Newswire, ABBOTT PARK, Ill., July 15, 2016
Abbott announced today that the U.S. Food and Drug Administration (FDA) has approved the Tecnis Symfony® Intraocular Lenses for the treatment of cataracts. The first in a new category of intraocular lenses (IOLs), the Tecnis Symfony lenses are the only lenses in the United States that provide a full range of continuous high-quality vision following cataract surgery, while also mitigating the effects of presbyopia by helping people focus on near objects. The FDA approval includes a version of the lens for people with astigmatism, the Tecnis Symfony Toric IOL.
Cataracts are a common condition, with almost 4 million cataract surgeries performed each year, and that number is expected to increase.1 By age 80, more than half of all Americans either have a cataract or have had cataract surgery.2 However, cataracts do not just impact seniors. In 2016 it is estimated that nearly one in four cataract surgeries will be performed on people younger than 65.1 Many people who have cataracts experience other problems with their vision, such as presbyopia and astigmatism, which the Symfony lenses also address. Presbyopia, which affects most people over age 40, means people have lost the ability to focus on objects up close and often require glasses to perform near visual tasks. Astigmatism is when the cornea is misshapen, which causes blurry or distorted vision.
“The Symfony intraocular lens is a new option I can offer my patients to improve their vision following cataract surgery, especially those who have difficulty focusing on objects at near distances because of presbyopia,” said Eric D. Donnenfeld, M.D., of Ophthalmic Consultants of Long Island, New York. “Many of my patients live very active lifestyles and want to see clearly at all distances, and without glasses if possible. With the Symfony lens, I can give patients the freedom to enjoy the activities that matter to them, while wearing glasses less.”
During cataract surgery, the natural lens of the eye is removed, and an artificial lens, called an intraocular lens, or IOL, is inserted into the eye. The IOL most commonly used in cataract surgery is a monofocal lens, which only allows the person to see at a distance, with closer objects being out of focus. In contrast, the Symfony lens was specifically developed with features to improve both the range and quality of vision.
“Abbott is focused on improving people’s vision and their lives by helping them stay healthy and active. Symfony offers patients, including those with astigmatism, an option for crisp, clear vision at all distances,” said Thomas Frinzi, senior vice president of Abbott’s vision business. “This is an important addition to our portfolio of lenses, as we expect many patients to choose a Symfony lens over a standard monofocal lens, given its benefits. We are happy that we can offer more people around the world this new category of lenses.”
The approval was based on results of a U.S. pivotal study that compared the Tecnis Symfony lens to a Tecnis aspheric monofocal lens in 298 patients. Compared with patients in the monofocal group, those who received a Tecnis Symfony IOL achieved greater improvements in intermediate and near vision while maintaining similar distance vision. Patients in the Symfony group were also more likely to achieve reduced overall spectacle wear and high overall visual performance in any lighting condition. Rates of adverse events did not differ between the Symfony and monofocal groups.
The Symfony lens is approved in more than 50 countries around the world, and has been widely studied, with data from numerous clinical studies involving over 2,000 eyes. In clinical studies, the Symfony lens:
- Provided seamless, day-to-night vision. Patients could see objects sharply and clearly at near, intermediate and far away distances, and points in between.
- Provided high-quality vision. Some IOLs may leave patients with an inability to focus clearly due to competing wavelengths of light passing through the lens at different angles (known as chromatic aberration), or with vision that is not completely focused because of the shape of the lens (known as spherical aberration). The Symfony lens has been engineered to correct these issues.
- Demonstrated a low incidence of halo and glare, which may be perceived as rings or blurring around bright lights. Glare and halo can sometimes affect an individual’s ability to drive at night or to perform other visual tasks.
INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR TECNIS SYMFONY AND TECNIS SYMFONY TORIC EXTENDED RANGE OF VISION IOLs
CAUTION: Federal law restricts this device to sale by or on the order of a physician.
INDICATIONS FOR USE: The TECNIS Symfony IOL, Model ZXR00, is indicated for primary implantation for the visual correction of aphakia in adult patients with less than 1 diopter of pre-existing corneal astigmatism in whom a cataractous lens has been removed. The lens mitigates the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, the lens provides improved intermediate and near visual acuity while maintaining comparable distance visual acuity. The Model ZXR00 IOL is intended for capsular bag placement only.
The TECNIS Symfony Toric IOLs, Models ZXT150, ZXT225, ZXT300 and ZXT375, are indicated for primary implantation for the visual correction of aphakia and for reduction of residual refractive astigmatism in adult patients with greater than or equal to 1 diopter of preoperative corneal astigmatism in whom a cataractous lens has been removed. The lens mitigates the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, the lens provides improved intermediate and near visual acuity while maintaining comparable distance visual acuity. The Model Series ZXT IOLs are intended for capsular bag placement only.
CONTRAINDICATIONS: None.
RISKS: Routine cataract surgery risks, irrelevant to lens selection, could be minor, temporary, or affect patients’ vision permanently. Rare complications are worsening of vision, bleeding, or infection. Risks related to use of this lens include a slight loss in vision sharpness with decreased use of glasses. Even with glasses, loss of sharpness may worsen under poor visibility conditions such as dim light or fog. This may lead to driving difficulties, and not detecting road hazards as quickly at night or in fog. Patients may also notice halos, starbursts, glare, and other visual symptoms with extended range of vision IOLs. This may impact patients when there are bright lights at night. Patients should discuss all risks and benefits with their eye doctor before surgery.
WARNINGS: A small number of patients may want their TECNIS Symfony IOL removed because of lens-related optical/visual symptoms. Patients with pre-existing diseases or conditions (i.e., diabetes and heart disease) may have higher risk of experiencing complications (e.g., more difficult recovery) after routine cataract surgery. Patients should not receive this lens if they have had previous trauma to their eye. Not evaluated for use in children.
PRECAUTIONS: If the patient’s eye is unhealthy (including glaucoma), vision may not be good even after cataract removal; patients may not get full benefit of the TECNIS IOL. Before surgery, the eye doctor will check for any eye diseases. Patients’ vision with the TECNIS Symfony IOL may not be good enough to perform detailed ‘up-close’ work without glasses, and rarely, may make some types of retinal treatment (e.g., retinal tear repair) more difficult. Patients should take all prescribed medicines and apply eye drops as instructed to avoid inflammation and infection. Patients should avoid bending down and playing sports, which can harm the eye during recovery. The eye doctor will tell patients what activities to avoid.
SERIOUS ADVERSE EVENTS: Serious adverse events observed during the TECNIS Symfony clinical trial were not related to the lenses. These events included swelling of the retina, inflammation and secondary surgeries.