More and more eye surgeons are concerned about the growing rate of Age-related macular degeneration (ARMD). ARMD is a leading cause of blindness in industrialized countries. ARMD is estimated to be responsible of 22.9% of the cases of blindness and 54.4% of visual impairments in the white American population [1].
As of 2018, 9.1 million Americans over the age of 50 are likely to suffer from an early ARMD [2]. This number is expected to double by 2050 to reach 17.8 million [3]. The severe visual loss due to ARMD is affecting at least 12% of the U.S. and European populations over the age of 80 [2], [4], [5].
Age, smoking, skin color, genetic/family risk factors and nutritional antioxidant deficiencies have been identified as risk factors in ARMD [6]. While controversial, I am concerned that blue light from electronic screens is a new key risk factor many are not aware of. Several studies indicate light exposure, particularly blue light, is a factor in the cause of ARMD [7], [8], [9], [10], [11], [12], [13].
Here is some data:
1. EUREYE study found significant association between blue light exposure and neovascular ARMD in individuals having the lowest antioxidant level [11].
2. Scientist studied 838 watermen of the Chesapeake Bay & showed that patients with advanced ARMD had significantly higher exposure to blue or visible light over the preceding 20 years [8].
3. An epidemiological study concerning the association between ARMD and sunlight exposure concluded that individuals with more sunlight exposure are at a significantly increased risk of ARMD [14].
4. Studies performed on animal and cellular models were able to demonstrate the toxicity of light and more specifically of the blue spectral range on the RPE and photoreceptor cells.
For instance,
in vivo (ie in an animal or living being) experiments revealed that photochemical damages exhibit lower dose thresholds in the UVs and in the blue range than for green or red light on the retina
[22] of monkey
[23],
[24], rat
[25],
[26],
[27] and rabbit
[28],
[29],
[30],
[31],
[32]. A greater toxicity of blue light was confirmed by exposing human RPE cells loaded with lipofuscin during 48 hours to blue-green light (390–550 nm, 2.8 mW/cm
2) compared to yellow-red light (550–800 nm, 2.8 mW/cm
2)
[34]. Similarly, exposure to blue light (480±20 nm, 75 mW/mm
2) induced more cell death on immortalized RPE cells loaded with A2E (ARPE-19 cell line) than green light (545±15 nm, 200 mW/mm
2)
[36]. Blue light-induced cell death was mediated by apoptotic processes involving caspase-3 and p-53 activation
[40],
[41]. However, in these studies, the light irradiance was not normalized to physiological conditions, meaning (i) no calibration on sunlight spectrum and (ii) no consideration for the eye media filtering. Furthermore, no test was achieved to precisely define the most toxic wavelengths within the entire blue range.
| Color |
Wavelength interval |
Frequency interval |
| Yellow |
~ 590–560 nm |
~ 510–540 THz |
| Green |
~ 560–520 nm |
~ 540–580 THz |
| Cyan |
~ 520–490 nm |
~ 580–610 THz |
| Blue |
~ 490–450 nm |
~ 610–670 THz
|
My Conclusion:
1. I am starting to use & recommend blue blocking glasses & screen protectors for your eyes.
2. Recommending Lux to decrease intensity of light on the computer.
More info and References below:
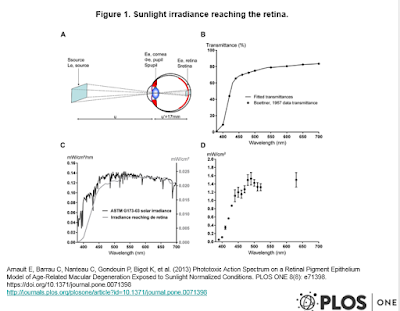
In the present study, our aim was first to calculate sunlight irradiances reaching the retina and second to assess on A2E-loaded RPE cells the light toxicity of 10 nm illumination bands at irradiances normalized to the calculated retinal sunlight irradiances. We have thus defined the most toxic wavelengths in the blue range, which could be precisely removed to best preserve color vision and non-visual functions.
In Vivo Studies: Macular damage was investigated under very intense light during a short period such as 3000 lux for up to 2 hours in albino rats. Photoreceptor degeneration occurred within less than 90 minutes whereas RPE cell apoptosis was delayed by several hours
[44]. The use of two different animal models rhodopsin and RPE65 deficient mice indicated that rhodopsin activation is required to trigger this photoreceptor degeneration
[45]. When different illumination bands were tested, blue light (403±10 nm) generated severe retinal damages whereas green light (550±10 nm) had no toxic effect
[25]. This toxic effect of blue light was attributed to the photoreversal of rhodopsin bleaching, which can occur under blue but not green light increasing thereby the photon catch capacity of the retina
[25]. This blue light damage of photoreceptor may therefore differ from the blue light damage of RPE cells. This conclusion was further supported by the observation of RPE cell death in blue light-exposed mice lacking rhodopsin
[25]. However, this
in vivo blue light damage of RPE cells could also differ from A2E-induced RPE cell damages because rhodopsin knockout mouse retina are unlikely to generate A2E formation as following RPE65 blockade
[46]. This
in vivo blue light damage of RPE cells could be more relevant to the RPE damage observed in our hands in the absence of A2E. However, the A2E-induced light damage of RPE cells could be relevant to the early RPE/photoreceptor dystrophy associated with light-induced photoreceptor degeneration recently described in mouse models with abnormal A2E accumulation
[47],
[48]. In fact, these mice were even considered animal models of ARMD as they display several major ARMD features such as lipofuscin accumulation, drusens, RPE cell death, complement activation and even choroidal neovascularization
[49]. Future studies should therefore investigate if the phototoxic action spectrum defined in our
in vitro study on A2E-loaded RPE cells is similarly more toxic during the light-induced degeneration in these ARMD animal models and whether filtering-out the corresponding wavelengths would efficiently prevent the RPE/photoreceptor degeneration and even suppress other complications.
Lux: The amount of light that is cast on a surface is called illuminance, which is measured in lux. This can be thought of as light intensity within a specific area.
Light involvement in the development of ARMD was suggested by epidemiological studies and by the beneficial influence of macular pigments as well as other antioxidants. Macular pigments are natural protective filters attenuating blue light in the range from 400 to 500 nm with peaks at 452 and 463 nm for lutein and zeaxanthin, respectively. Their absorptions and thus, their retinal concentrations, are known to decrease with age
[50],
[51],
[52]. So, their high level dietary supplementation might diminish the risk of late ARMD
[53] and even improve visual functions in severe ARMD patients
[54]. All these conclusions are consistent with a mechanism of light-induced toxicity in the blue light range. In fact, this natural protection has been used to generate broad blue blocking filters and intraocular lenses
[55],
[56],
[57],
[58]. However, if the ARMD physiopathology relies on A2E photosensitization, our result suggests that filtering light in a narrower band from 415 nm to 455 nm may be sufficient to prevent or limit the disease development or progression. This more precise and narrower phototoxic action spectrum could be advantageously valued in selective photoprotection ophthalmic filters which would limit the disruption of color vision and of non-visual functions, by contrast to current blue filtering intraocular lenses
[59]. Indeed, filters in our narrow bandwidth would not occlude light in the 460–500 nm range, not only essential for color vision but also for pupil constriction and circadian rhythm regulation, both mediated by melanopsin-sensitive retinal ganglion cells. Future studies will therefore have to evaluate if new selective ophthalmic filters in the here defined bandwidth from 415 nm to 455 nm could provide macular protection in patients at risk for ARMD.
1. Abstract
Among the identified risk factors of age-related macular degeneration, sunlight is known to induce cumulative damage to the retina. A photosensitive derivative of the visual pigment, N-retinylidene-N-retinylethanolamine (A2E), may be involved in this phototoxicity. The high energy visible light between 380 nm and 500 nm (blue light) is incriminated. Our aim was to define the most toxic wavelengths in the blue-green range on an in vitro model of the disease. Primary cultures of porcine retinal pigment epithelium cells were incubated for 6 hours with different A2E concentrations and exposed for 18 hours to 10 nm illumination bands centered from 380 to 520 nm in 10 nm increments. Light irradiances were normalized with respect to the natural sunlight reaching the retina. Six hours after light exposure, cell viability, necrosis and apoptosis were assessed using the Apotox-Glo Triplex™ assay. Retinal pigment epithelium cells incubated with A2E displayed fluorescent bodies within the cytoplasm. Their absorption and emission spectra were similar to those of A2E. Exposure to 10 nm illumination bands induced a loss in cell viability with a dose dependence upon A2E concentrations. Irrespective of A2E concentration, the loss of cell viability was maximal for wavelengths from 415 to 455 nm. Cell viability decrease was correlated to an increase in cell apoptosis indicated by caspase-3/7 activities in the same spectral range. No light-elicited necrosis was measured as compared to control cells maintained in darkness. Our results defined the precise spectrum of light retinal toxicity in physiological irradiance conditions on an in vitro model of age-related macular degeneration. Surprisingly, a narrow bandwidth in blue light generated the greatest phototoxic risk to retinal pigment epithelium cells. This phototoxic spectrum may be advantageously valued in designing selective photoprotection ophthalmic filters, without disrupting essential visual and non-visual functions of the eye.
3.
“High Energy Visible (HEV) blue light has been identified for years as the most dangerous light for the retina. After chronic exposure, one can expect to see long range growth in the number of macular degenerations, glaucomas, and retinal degenerative diseases”. And a paper published by the American Macular Degeneration Foundation (AMDF) reported that “the blue rays of the spectrum seem to accelerate age-related macular degeneration (AMD) more than any other rays in the spectrum”. In addition, a report by the Beaver Dam Eye Study showed that “increased exposure to blue light in the teens, 20s, and 30s increased the risk of onset age AMD by 10 years, effectively doubling the chances of blindness during lifetime.”
A pair of glasses might be labeled UV absorbent, for example, but the label might not indicate exactly how much UVA and UVB rays are blocked. Sunglasses should be labeled UV 400.
References:
References
- 1.Congdon N, O’Colmain B, Klaver CC, Klein R, Munoz B, et al. (2004) Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol 122: 477–485.
- 2.Friedman DS, O’Colmain BJ, Munoz B, Tomany SC, McCarty C, et al. (2004) Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol 122: 564–572.
- 3.Rein DB, Wittenborn JS, Zhang X, Honeycutt AA, Lesesne SB, et al. (2009) Forecasting age-related macular degeneration through the year 2050: the potential impact of new treatments. Arch Ophthalmol 127: 533–540.
- 4.Smith W, Assink J, Klein R, Mitchell P, Klaver CC, et al. (2001) Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology 108: 697–704.
- 5.Augood CA, Vingerling JR, de Jong PT, Chakravarthy U, Seland J, et al. (2006) Prevalence of age-related maculopathy in older Europeans: the European Eye Study (EUREYE). Arch Ophthalmol 124: 529–535.
- 6.Seddon JM, Reynolds R, Yu Y, Daly MJ, Rosner B (2012) Risk models for progression to advanced age-related macular degeneration using demographic, environmental, genetic, and ocular factors. Ophthalmology 118: 2203–2211.
- 7.Cruickshanks KJ, Klein R, Klein BE, Nondahl DM (2001) Sunlight and the 5-year incidence of early age-related maculopathy: the beaver dam eye study. Arch Ophthalmol 119: 246–250.
- 8.Taylor HR, West S, Munoz B, Rosenthal FS, Bressler SB, et al. (1992) The long-term effects of visible light on the eye. Arch Ophthalmol 110: 99–104.
-
January 1992
The Long-term Effects of Visible Light on the Eye
Arch Ophthalmol. 1992;110(1):99-104. doi:10.1001/archopht.1992.01080130101035
FullText
• The relationship between exposure to sunlight and senile cataract, age-related macular degeneration, pterygium, and climatic droplet keratopathy was examined in 838 watermen who work on the Chesapeake Bay. The presence and severity of lenticular, corneal, and macular changes were assessed by either clinical examination or from stereo macular photographs. From detailed exposure histories, ocular exposure was estimated for three bands of visible radiation—violet (400 to 450 nm), blue (400 to 500 nm), or all visible (400 to 700 nm)—as well as for UV-A (320 to 340 nm) and UV-B (290 to 320 nm). The results with each band of visible radiation were similar. Neither cortical nor nuclear cataract was associated with ocular exposure to blue or all visible radiation, but pterygium and climatic droplet keratopathy were more common with higher exposures. Compared with age-matched controls, patients with advanced age-related macular degeneration (geographic atrophy or disciform scarring) had significantly higher exposure to blue or visible light over the preceding 20 years (odds ratio, 1.36 [1.00 to 1.85]) but were not different in respect to exposure to UV-A or UV-B. These data suggest that high levels of exposure to blue or visible light may cause ocular damage, especially later in life, and may be related to the development of age-related macular degeneration.
-
9.
- Young RW (1992) Sunlight and age-related eye disease. J Natl Med Assoc 84: 353–358.
- 10.Mitchell P, Smith W, Wang JJ (1998) Iris color, skin sun sensitivity, and age-related maculopathy. The Blue Mountains Eye Study. Ophthalmology 105: 1359–1363.
- 11.Fletcher AE, Bentham GC, Agnew M, Young IS, Augood C, et al. (2008) Sunlight exposure, antioxidants, and age-related macular degeneration. Arch Ophthalmol 126: 1396–1403.
- 12.Butt AL, Lee ET, Klein R, Russell D, Ogola G, et al. (2011) Prevalence and risks factors of age-related macular degeneration in Oklahoma Indians: the Vision Keepers Study. Ophthalmology 118: 1380–1385.
- 13.Vojnikovic B, Synek S, Micovic V, Telezar M, Linsak Z (2010) Epidemiological study of sun exposure and visual field damage in children in Primorsko-Goranska County – the risk factors of earlier development of macular degeneration. Coll Antropol 34 Suppl 257–59.
- 14.Sui GY, Liu GC, Liu GY, Gao YY, Deng Y, et al. (2013) Is sunlight exposure a risk factor for age-related macular degeneration? A systematic review and meta-analysis. Br J Ophthalmol. 97: 389–394.
- 15.Klein R, Cruickshanks KJ, Nash SD, Krantz EM, Javier Nieto F, et al. (2010) The prevalence of age-related macular degeneration and associated risk factors. Arch Ophthalmol 128: 750–758.
- 16.Bazan HE, Bazan NG, Feeney-Burns L, Berman ER (1990) Lipids in human lipofuscin-enriched subcellular fractions of two age populations. Comparison with rod outer segments and neural retina. Invest Ophthalmol Vis Sci 31: 1433–1443.
- 17.Ng KP, Gugiu B, Renganathan K, Davies MW, Gu X, et al. (2008) Retinal pigment epithelium lipofuscin proteomics. Mol Cell Proteomics 7: 1397–1405.
- 18.Sparrow JR, Wu Y, Kim CY, Zhou J (2010) Phospholipid meets all-trans-retinal: the making of RPE bisretinoids. J Lipid Res 51: 247–261.
- 19.Ben-Shabat S, Itagaki Y, Jockusch S, Sparrow JR, Turro NJ, et al. (2002) Formation of a nonaoxirane from A2E, a lipofuscin fluorophore related to macular degeneration, and evidence of singlet oxygen involvement. Angew Chem Int Ed Engl 41: 814–817.
2.
Blue Light
Recent studies suggest that the blue end of the light spectrum may also contribute to retinal damage and possibly lead to AMD. The retina can be harmed by high-energy visible radiation of blue/violet light that penetrates the macular pigment found in the eye. According to a study by The Schepens Eye Institute, a low density of macular pigment may represent a risk factor for AMD by permitting greater blue light damage.
Harmful Effects of Ultra-violet and Blue Light Ultra-violet light is that portion of the spectrum of invisible light below 286nm to 400nm, and is generally understood to be harmful to the eye, possibly leading to cataracts and other eye diseases such as age-related macular degeneration (AMD). Retinal damage is the most important hazard from light. The three types of retinal damage are structural, thermal and photochemical. The type of damage depends on the wavelength, power level and exposure time.
Sources of UV Light
While the primary source of UV light is the sun, other sources include welder’s flash, video display terminals, fluorescent lighting, highintensity mercury vapor lamps (for night sports and high-crime areas), and xenon arc lamps.
Types of UV Light
UV light is divided into three segments, which are designated as A, B, and C, described briefly below in order from least harmful to most harmful to the eye.
- UVC (below 286nm) is effectively filtered by the earth’s ozone layer.
- UVB (286-320nm) is that solar energy which is the cause of sunburn and snow blindness and is absorbed by the cornea.
- UVA (320-400nm) is that part of the invisible spectrum of particular concern to eye care professionals. It is the most damaging of UV radiation, and it is the radiation transmitted to the crystalline lens of the human eye.
Melanin as Protection from Harmful UV Light
Researchers have identified melanin as the substance in the skin, hair and eyes that absorbs harmful UV and blue light. It is the body’s natural sunscreen protection. Higher amounts of melanin afford greater protection against damaging light rays, but melanin is lost as we age. By age 65, about half of the protection is gone, increasing susceptibility to eye disease such as macular degeneration. The Schepens Eye Institute reports that “the blue rays of the spectrum seem to accelerate AMD more than other rays of the spectrum.” Very bright lights such as sunlight or its reflection in the ocean or desert may worsen macular degeneration. The Institute recommends that sunglasses protect against both blue/violet and UV light.
By including synthetic melanin in our sunglasses, we may be compensating for the melanin lost as we age. With such sunglasses, the colors are filtered in proportion to their damage potential, and thus the danger of macular degeneration may be reduced. Many optical shops that sell prescription eyewear now have melanin lenses available. For an online source, see
Melanin Products from PhotoProtective Technologies, the inventors of melanin lenses.
Who needs protection from harmful UV light? – Those who work or play in the sun. For example, construction workers, farmers, truck drivers, sports participants and spectators, police officers, skiers, lifeguards, and beach goers.
Who else? Those in certain light environments. For example, if you work in an environment which is brightly lit with fluorescent light fixtures or if you spend hours in front of a computer terminal.
Anyone else? – Those taking medications! There are many photosensitizing drugs on the market today, including certain tranquilizers, diuretics, oral contraceptives, antibiotics, anti-diabetic and anti-hypertensive medications, and even artificial sweeteners such as cyclamates.
Guidelines on UV Protective Eyewear
AMDF Web site visitors are advised to protect their eyes from potentially harmful UV light. Not only is harmful UV light present on sunny days, it is also present on overcast or hazy days. UV protection is available for clear lenses as well as sunglasses. The UV protection that is available is an invisible coating that doesn’t change the color of the eyeglass lens.
Misleading claims about certain glasses providing UV protection can be easily confusing to consumers. A pair of glasses might be labeled UV absorbent, for example, but the label might not indicate exactly how much UVA and UVB rays are blocked. Sunglasses should be labeled UV 400. It is recommended that you protect yourself from UV radiation up to 400 nanometers, which extends into part of the visible spectrum to ensure complete blockage of ultraviolet light. This is what distinguishes “cheap” sunglasses from more expensive ones.
Ask your eyecare professional if your eyewear has been treated for UV light protection. He or she will be glad to answer your questions and ensure that your eyes are adequately protected from UV radiation damage. Melanin lenses are now readily available at most optical shops which sell prescription eyewear.

![uv_eye2[1]](https://www.macular.org/wp-content/uploads/2016/05/uv_eye21-300x84.jpg)